This article would not exist without the laboratory environment in which its central idea first took shape. I owe particular gratitude to my supervisor at Brigham and Women’s Hospital, Dr Tanya Laidlaw whose meticulous approach to blood processing in our clinical trial laboratory first drew my attention to the scientific significance of centrifugation as an act of precision rather than mere procedure. What began as careful observation became the intellectual foundation of this manuscript.
I am grateful to the patients who participated in the AERD clinical research that forms the context of this work. Their willingness to contribute biological specimens to science represents a form of generosity that laboratory professionals carry a responsibility to honour through careful handling.
I also wish to acknowledge the broader community of clinical laboratory scientists whose daily discipline sustains the reliability of biomedical evidence — often without recognition.
Clinical laboratories are often perceived as silent spaces operating behind the visible machinery of medicine. Patients rarely witness what happens after blood leaves the body. Physicians may review the final laboratory values, researchers may interpret the datasets, and pharmaceutical sponsors may observe statistical outputs within clinical trials, yet the operational reality of laboratory processing itself remains largely invisible. Beneath every biomarker, cytokine profile, inflammatory panel, and immunological dataset lies a chain of human handling, procedural precision, centrifugation timing, and analytical judgement that fundamentally shapes the quality of scientific evidence produced.
This book emerged from direct observation within the clinical trial laboratory environment, particularly within allergy and immunology research involving Aspirin-Exacerbated Respiratory Disease (AERD). While much scientific attention is often devoted to downstream analytical platforms, molecular technologies, statistical modelling, and therapeutic outcomes, comparatively less attention is directed toward the pre-analytical phase of blood handling. Yet in many cases, the quality of the final dataset is determined long before laboratory instruments generate measurable outputs. The integrity of blood processing itself becomes an unseen determinant of scientific validity.
Among the most operationally underestimated processes within laboratory workflows is centrifugation. The act of spinning blood may initially appear routine and mechanical. However, repeated centrifugation, particularly through double-spin or triple-spin approaches, can substantially influence plasma clarity, cellular separation, particulate reduction, and ultimately biomarker detectability. In highly sensitive immunological investigations, especially those involving inflammatory disease pathways, even minor residual cellular interference may alter downstream analytical resolution.
Within AERD-related clinical research, where inflammatory signalling pathways are biologically complex and highly dynamic, the reliability of immunological measurements becomes critically important. Cytokines, eosinophilic markers, leukotrienes, immunoglobulins, and inflammatory mediators may be affected not only by disease progression or therapeutic intervention but also by sample handling conditions prior to analysis. Consequently, laboratory operations should not be viewed merely as supportive administrative functions but rather as active scientific infrastructures participating directly in data generation itself.
This book explores the concept of large component adjustment through repeated centrifugation as a form of pre-analytical data enhancement. The term “large component adjustment” within this context refers to the refinement of blood-derived sample quality through the progressive reduction of residual cellular materials, platelets, particulate matter, and separation inconsistencies that may interfere with downstream immunological analysis. Rather than treating centrifugation as a fixed procedural step, this book examines repeated spinning as a deliberate optimisation strategy capable of improving analytical sensitivity and dataset consistency within clinical trial environments.
The discussion throughout this book integrates scientific reasoning, operational laboratory experience, immunological theory, and clinical trial methodology. The objective is not merely to explain centrifugation mechanics but to situate blood processing within the broader architecture of translational medicine. Laboratory procedures influence biomarker reliability. Biomarker reliability influences clinical interpretation. Clinical interpretation influences therapeutic development. Thus, operational laboratory precision contributes directly to the production of medical knowledge itself.
Importantly, this book also seeks to humanise laboratory work. Clinical laboratories are frequently associated with automation, instrumentation, and standard operating procedures, yet laboratory science remains deeply dependent upon human observation, timing, discipline, and consistency. Behind every processed sample exists a network of laboratory personnel navigating procedural complexity under strict regulatory and temporal constraints. Scientific reproducibility is therefore not solely technological but operational and human.
The structure of this book reflects this interdisciplinary perspective. Early chapters establish the scientific foundations of blood composition, immunological signalling, allergy research, and AERD pathophysiology. Subsequent chapters examine centrifugation theory, repeated spinning methodologies, plasma refinement strategies, and biomarker sensitivity. Later sections investigate clinical trial implications, operational laboratory challenges, governance considerations, and the future of immunological blood analytics within precision medicine systems.
Although this book is grounded in clinical laboratory practice, its broader argument extends beyond technical methodology. It argues that pre-analytical optimisation deserves greater scientific recognition within biomedical research ecosystems. In an era increasingly driven by precision medicine, artificial intelligence, high-resolution biomarker analysis, and personalised therapeutics, the importance of sample integrity will continue to expand. Advanced analytical technologies cannot compensate fully for compromised biological inputs. The quality of scientific interpretation remains inseparable from the quality of laboratory preparation.
Ultimately, this work positions laboratory blood processing not as an invisible background procedure but as a scientific intervention capable of shaping the reliability, interpretability, and translational value of clinical research itself.
UNDERSTANDING BLOOD AS BIOLOGICAL DATA
Blood is frequently understood within medicine as a diagnostic substance used to identify disease, monitor physiological abnormalities, and evaluate therapeutic response. However, within clinical trial environments, blood functions as something far more complex than a routine diagnostic specimen. Blood operates simultaneously as a biological archive, a molecular communication system, an immunological map, and a dynamic source of measurable scientific data. Every millilitre of collected blood contains layers of physiological information reflecting interactions between cellular systems, inflammatory pathways, immune responses, metabolic regulation, and environmental exposures.
Within allergy and immunology research, blood serves as a particularly important analytical medium because immune activity is fundamentally systemic. Cytokines circulate throughout plasma. Eosinophils migrate across inflammatory environments. Immunoglobulins interact with allergens and signalling molecules. Platelets contribute not only to coagulation but also to inflammatory modulation. Consequently, the composition of blood becomes a continuously evolving representation of immunological behaviour occurring throughout the body. (Gros et al., 2014; Semple et al., 2011)
From a laboratory perspective, blood is not biologically static after collection. Immediately following venepuncture, biological degradation processes begin to emerge. Cellular metabolism continues temporarily outside the body. Platelets may become activated. White blood cells may release intracellular substances. Protein integrity may gradually deteriorate under improper handling conditions. Delays in processing, temperature instability, mechanical disruption, and inconsistent centrifugation may all influence the quality of downstream analytical measurements. (Lippi et al., 2011; Flower et al., 2000)
For this reason, the pre-analytical phase of laboratory processing occupies a critical position within clinical trial science. The pre-analytical phase includes all procedures occurring before formal laboratory analysis itself, including collection timing, tube selection, inversion protocols, transport conditions, centrifugation, plasma separation, aliquoting, storage, and handling consistency. Although often overshadowed by analytical instrumentation and statistical methodologies, the pre-analytical phase may contribute significantly to laboratory variability. (Lippi et al., 2011)
In many clinical studies, researchers focus heavily on assay sensitivity, molecular technologies, or statistical interpretation while underestimating the extent to which sample preparation shapes final data quality. Yet analytical systems can only evaluate the biological integrity of the sample they receive. Even highly advanced immunological platforms may produce distorted outputs if residual cellular contamination, platelet interference, haemolysis, or inflammatory artefacts remain present within inadequately processed plasma. (Plebani, 2006)
The relationship between blood processing and data reliability becomes especially important in inflammatory disease research. In conditions involving chronic immune activation, including AERD, biomarker concentrations may already exist within narrow measurable ranges. Small procedural inconsistencies may therefore generate disproportionately large interpretational consequences. Residual inflammatory cells remaining within plasma after incomplete separation may continue releasing cytokines or inflammatory mediators during storage or transport, thereby altering measured concentrations independently of actual patient physiology.
Understanding blood as biological data therefore requires understanding that data integrity begins operationally, not statistically. The centrifuge becomes more than a mechanical instrument for separating components. It becomes part of the scientific architecture responsible for preserving interpretational accuracy. Repeated spinning strategies emerge within this context not merely as procedural repetition but as attempts to refine biological signal quality through improved sample purification and component isolation.
Blood itself contains multiple major components, each contributing differently to laboratory analysis. Plasma serves as the liquid matrix carrying proteins, hormones, cytokines, antibodies, electrolytes, and inflammatory mediators. Red blood cells dominate volumetric composition but are generally removed for plasma-based immunological assays. White blood cells participate directly in immune regulation and inflammatory signalling. Platelets contribute to coagulation while also interacting with immune pathways and inflammatory mechanisms.
Following centrifugation, these components separate according to density. Red blood cells settle at the bottom of the tube due to their relatively greater mass. Plasma remains at the upper layer. Between these layers forms the buffy coat, a thin intermediate region containing leukocytes and platelets. The precision with which these layers separate significantly affects plasma purity and downstream analytical reliability.
Single-spin centrifugation may successfully isolate basic plasma fractions for routine laboratory applications. However, within sensitive immunological research, residual platelets, microcellular debris, or incomplete separation may persist despite initial spinning. These residual materials can introduce analytical noise into cytokine measurements, inflammatory assays, and biomarker evaluations. Consequently, some laboratory protocols adopt repeated centrifugation approaches to further refine plasma quality.
The concept of large component adjustment emerges from this operational objective. By repeatedly spinning plasma under controlled conditions, laboratories may progressively reduce residual particulates and improve separation consistency. The second or third spin therefore functions as a refinement mechanism designed to enhance sample clarity, improve biomarker stability, and reduce pre-analytical variability.
Importantly, this process should not be understood as merely technical optimisation detached from broader scientific outcomes. Clinical trial data influence therapeutic approvals, treatment recommendations, and scientific understanding of disease mechanisms. Thus, procedural refinements affecting laboratory reliability may ultimately influence medical decision-making itself.
The modern clinical laboratory therefore occupies a strategic position within translational medicine. Laboratories no longer function solely as diagnostic support facilities but increasingly serve as data-generation infrastructures underpinning biomedical innovation. As precision medicine advances and biomarker-driven therapeutics expand, the quality of laboratory processing will become increasingly inseparable from the quality of scientific discovery.
ALLERGY, IMMUNOLOGY, AND AERD
The immune system exists as one of the most sophisticated regulatory systems within the human body. Unlike isolated physiological structures performing singular functions, the immune system operates through highly interconnected signalling networks involving cellular communication, inflammatory regulation, tissue surveillance, and biochemical coordination. Its primary purpose is protection. However, within allergic and inflammatory diseases, the same protective mechanisms designed to preserve physiological stability may become dysregulated, exaggerated, or chronically activated. The consequence is not merely temporary inflammation but a persistent alteration in immune behaviour capable of affecting multiple organ systems simultaneously.
Allergy and immunology research therefore examines more than hypersensitivity reactions alone. It investigates the broader mechanisms through which immune signalling pathways influence disease progression, inflammatory persistence, respiratory function, tissue remodelling, and therapeutic response. Blood analysis becomes central within this field because immunological activity frequently leaves measurable biological signatures circulating throughout the bloodstream. Cytokines, eosinophils, leukotrienes, chemokines, immunoglobulins, and inflammatory mediators collectively provide insight into the state of immune activation occurring within the body.
Among the more complex inflammatory conditions studied within allergy and immunology is Aspirin-Exacerbated Respiratory Disease (AERD). AERD represents a chronic inflammatory disorder characterised by asthma, nasal polyposis, chronic sinus disease, and hypersensitivity reactions to aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs). Although clinically recognised for decades, AERD remains biologically intricate because its pathophysiology involves overlapping inflammatory pathways rather than a single isolated mechanism. (Laidlaw & Boyce, 2016; Bochenek et al., 1996)
Patients with AERD frequently exhibit persistent eosinophilic inflammation together with dysregulated arachidonic acid metabolism and excessive leukotriene production. Under normal physiological conditions, arachidonic acid pathways contribute to inflammatory regulation through balanced production of prostaglandins and leukotrienes. In AERD, however, this balance becomes disrupted. The inhibition of cyclooxygenase-1 (COX-1) pathways following aspirin exposure reduces protective prostaglandin synthesis while simultaneously amplifying pro-inflammatory leukotriene activity. The result is intensified respiratory inflammation capable of triggering bronchospasm, airway obstruction, and systemic inflammatory responses. (Cahill & Boyce, 2014)
This inflammatory dysregulation extends beyond isolated respiratory symptoms. AERD often reflects broader immunological instability involving mast cell activation, eosinophilic recruitment, cytokine signalling abnormalities, and chronic mucosal inflammation. Consequently, the disease provides a particularly important model for studying inflammatory biomarkers within clinical trial environments. (Stevens et al., 2016; Cahill & Boyce, 2014)
Within AERD clinical research, blood samples become essential analytical resources because they allow investigators to evaluate inflammatory behaviour in measurable biochemical terms. Researchers may examine eosinophil counts, interleukin concentrations, prostaglandin metabolites, leukotriene activity, immunoglobulin levels, platelet interactions, and inflammatory protein expression. These measurements help determine disease severity, therapeutic response, inflammatory progression, and treatment efficacy.
However, the complexity of inflammatory signalling within AERD simultaneously creates analytical challenges. Many biomarkers relevant to allergy and immunology exist at relatively low measurable concentrations or fluctuate dynamically depending upon inflammatory state, medication exposure, timing, and biological variability. Cytokine concentrations may shift rapidly over short periods. Leukocyte activation may continue during sample handling. Platelets may release inflammatory mediators following improper processing conditions. Consequently, even minor inconsistencies within pre-analytical workflows may influence biomarker reliability. (de Jager et al., 2009; Aziz et al., 1999)
This is where laboratory operations become scientifically significant. In many forms of biomedical research, laboratory procedures are viewed primarily as standardised technical routines designed to support analytical systems. Yet within highly sensitive immunological investigations, laboratory handling itself may directly influence measurable inflammatory outputs. The distinction between biological signal and procedural artefact becomes increasingly important.
For example, incomplete plasma separation following centrifugation may allow residual platelets or leukocytes to remain suspended within plasma samples. These residual cellular materials may continue metabolically active processes after collection, releasing cytokines or inflammatory molecules that artificially alter measured biomarker concentrations. Similarly, haemolysis caused by mechanical disruption during handling may release intracellular contents into plasma, further compromising analytical specificity. (Flower et al., 2000; Aziz et al., 1999)
Repeated centrifugation strategies attempt to reduce these forms of interference. By performing secondary or tertiary spins under controlled conditions, laboratory personnel may improve plasma clarity and reduce residual particulate contamination. The objective is not aesthetic purity alone but analytical refinement. Cleaner plasma potentially allows more accurate measurement of inflammatory biomarkers central to AERD research.
Within immunology laboratories, centrifugation therefore becomes closely connected to the concept of signal preservation. Every blood sample contains both desired analytical signals and unwanted biological noise. Desired signals include measurable biomarkers reflecting true patient physiology. Biological noise may include cellular debris, platelet fragments, microclots, residual inflammatory cells, lipids, or mechanically induced artefacts introduced during handling. Large component adjustment through repeated spinning seeks to reduce this noise while preserving meaningful biological information.
The significance of this process increases within clinical trial settings because therapeutic outcomes frequently depend upon highly sensitive statistical comparisons. A small change in cytokine concentration may influence interpretations regarding drug efficacy, inflammatory suppression, or treatment response. If biomarker variability originates partly from inconsistent laboratory preparation rather than actual patient physiology, scientific conclusions may become distorted.
Clinical trial laboratories therefore operate under extensive procedural governance systems designed to minimise variability. Standard operating procedures specify centrifugation speeds, durations, temperatures, storage conditions, aliquoting methods, transport timelines, and chain-of-custody requirements. Yet even under tightly controlled protocols, operational judgement remains important. Laboratory personnel must frequently navigate practical realities including variable sample conditions, time-sensitive workflows, equipment limitations, and processing prioritisation under clinical constraints.
Importantly, allergy and immunology laboratories also occupy a unique intersection between patient biology and pharmaceutical development. Biomarker data generated within these environments contribute not only to academic understanding but also to therapeutic innovation. Clinical trials investigating biologics, anti-inflammatory agents, leukotriene modifiers, or immunomodulatory therapies rely heavily upon laboratory evidence demonstrating measurable immunological effects. Consequently, the quality of blood processing may indirectly influence broader translational medicine outcomes.
The immunological complexity of AERD further reinforces the importance of operational precision. Unlike diseases involving singular biomarkers, AERD reflects interacting inflammatory networks involving eosinophils, mast cells, platelets, prostaglandins, leukotrienes, and multiple cytokine systems simultaneously. This multidimensional inflammatory architecture requires analytical consistency capable of preserving subtle biological relationships across datasets.
Understanding AERD therefore requires understanding not only disease biology but also the laboratory infrastructures through which disease biology becomes measurable. Scientific interpretation depends upon operational integrity. Immunological insight depends upon sample stability. Biomarker reliability depends upon pre-analytical precision.
Within this framework, repeated centrifugation emerges not as unnecessary repetition but as a strategic refinement process situated within the broader pursuit of scientific reliability. The second spin becomes more than an operational step. It becomes an attempt to preserve the integrity of biological truth before analysis even begins.
THE CLINICAL TRIAL LABORATORY AS A SCIENTIFIC SYSTEM
Modern medicine is often publicly associated with physicians, hospitals, surgical technologies, pharmaceutical innovation, and visible patient care. Yet beneath the visible structure of healthcare exists another ecosystem operating with equal importance but substantially less recognition: the clinical trial laboratory. Clinical laboratories occupy a foundational position within biomedical research because they transform biological materials into measurable scientific evidence. Every therapeutic claim, biomarker analysis, immunological interpretation, and pharmaceutical conclusion emerging from clinical research is dependent upon the reliability of laboratory-generated data.
Within clinical trial environments, laboratories do not merely support science. They actively produce science.
This distinction is important because laboratory work is frequently misunderstood as passive technical processing rather than active scientific infrastructure. Blood arrives in collection tubes appearing deceptively simple and uniform. However, each sample contains highly dynamic biological systems vulnerable to degradation, contamination, inflammatory alteration, and procedural variability. The responsibility of the clinical trial laboratory is therefore not simply to process samples mechanically but to preserve biological integrity long enough for meaningful scientific interpretation to occur.
This challenge becomes especially significant within allergy and immunology research involving diseases such as Aspirin-Exacerbated Respiratory Disease (AERD). Inflammatory diseases are biologically unstable by nature. Cytokine concentrations fluctuate dynamically. Immune cells remain metabolically active. Platelets interact with inflammatory pathways. Biomarkers may exist at extremely low detectable concentrations. Consequently, the laboratory environment becomes a highly controlled operational system designed to minimise artificial disturbances that may interfere with biological signal preservation.
The public often imagines laboratory science as a fully automated process dominated entirely by sophisticated machinery. While automation has indeed transformed many analytical workflows, the reality of clinical trial laboratories remains deeply human. Human judgement, timing, observation, coordination, and procedural discipline remain essential at nearly every stage of blood handling. Scientific reliability therefore emerges not solely from technological sophistication but from operational consistency.
The journey of a blood sample through a clinical trial laboratory is considerably more complex than most outside the field realise. Before any centrifugation occurs, multiple variables already begin influencing sample stability. Patient preparation itself may affect biomarker readings. Fasting conditions, medication exposure, hydration status, circadian rhythms, inflammatory state, stress responses, and timing relative to therapeutic administration all influence the physiological composition of blood before collection even begins.
Following venepuncture, additional layers of complexity emerge immediately. The selection of collection tubes becomes scientifically relevant because different anticoagulants interact differently with downstream analytical systems. EDTA tubes preserve cellular morphology but may interfere with certain assays. Heparinised plasma may behave differently from serum. Sodium citrate influences coagulation-related measurements. The choice of collection medium therefore shapes analytical compatibility. (Bowen & Remaley, 2014)
Even the simple act of tube inversion after blood collection carries importance. Insufficient inversion may result in clot formation, while overly aggressive mixing may contribute to haemolysis. Small procedural inconsistencies at this stage can cascade throughout the entire analytical process. What appears operationally minor may become scientifically consequential. (Rai et al., 2005)
Transportation introduces another critical vulnerability period. Blood samples are biologically active systems temporarily existing outside physiological regulation. Delays in transport may allow ongoing cellular metabolism. Improper temperatures may destabilise proteins or cytokines. Mechanical agitation during handling may activate platelets or damage fragile cellular structures. Exposure to environmental conditions therefore becomes another source of potential pre-analytical variability.
Within clinical trial laboratories, timing is often treated with extraordinary precision because biological degradation does not pause while operational workflows adjust. Samples frequently arrive in waves corresponding to patient appointments, therapeutic schedules, or trial timelines. Laboratory personnel must coordinate centrifugation schedules, aliquoting procedures, freezer storage preparation, documentation protocols, and chain-of-custody verification simultaneously under strict temporal constraints.
In highly regulated clinical trials, every sample becomes traceable through extensive procedural documentation systems. Labels, timestamps, accession numbers, freezer logs, centrifugation records, temperature monitoring systems, and transport tracking collectively create an operational audit trail designed to preserve regulatory compliance and scientific accountability. These systems exist because clinical trial data may ultimately influence therapeutic approvals, pharmaceutical decisions, and patient treatment pathways internationally. (Moore et al., 2011)
Within this broader framework, centrifugation emerges as one of the most operationally significant procedures in laboratory medicine. The centrifuge functions not merely as a mechanical separator but as a scientific gatekeeper determining the quality of biological isolation achieved before downstream analysis.
At a fundamental level, centrifugation operates through centrifugal force generated by high-speed rotational motion. When blood samples spin at controlled revolutions per minute (RPM), components separate according to density. Red blood cells migrate downward due to their relatively greater mass. Plasma remains above as the lighter liquid fraction. Between these layers forms the buffy coat, containing leukocytes and platelets.
However, the theoretical simplicity of separation differs substantially from operational reality.
Blood is not a perfectly uniform substance. Samples vary between patients depending upon inflammatory state, lipid concentration, medication exposure, disease severity, hydration status, coagulation tendencies, and numerous physiological factors. Some samples separate cleanly after a single centrifugation cycle, while others retain residual cloudiness, platelet contamination, or microscopic particulate matter despite standard processing.
This variability becomes especially relevant within immunological and inflammatory disease research. Residual platelets suspended within plasma are not biologically inert. Platelets actively participate in inflammatory signalling and may release cytokines, chemokines, and bioactive mediators capable of influencing downstream assay measurements. Similarly, residual leukocytes may continue metabolic activity after collection, potentially altering cytokine concentrations during storage or transport. (Gros et al., 2014; Semple et al., 2011)
The concept of large component adjustment through repeated spinning emerges directly from these operational realities.
Repeated centrifugation seeks to improve plasma refinement beyond what may be achieved during a single spin alone. Following initial separation, plasma may undergo secondary or tertiary centrifugation cycles designed to remove remaining particulates, platelets, cellular fragments, fibrin residues, or microdebris. Each additional spin functions as a progressive purification step intended to improve analytical clarity.
Importantly, the rationale for repeated spinning is not cosmetic. Clearer plasma visually reflects improved component separation, but the true objective is analytical optimisation. Reduced biological interference may improve assay sensitivity, biomarker stability, reproducibility, and signal-to-noise resolution during downstream immunological analysis.
The phrase “signal-to-noise ratio” becomes particularly important within clinical laboratory science. Desired biological signals include measurable inflammatory markers genuinely reflecting patient physiology. Noise refers to unwanted procedural or biological interference capable of obscuring analytical interpretation. Residual platelets, haemolysis, lipaemia, microclots, and cellular debris all contribute forms of analytical noise.
In diseases involving subtle inflammatory fluctuations such as AERD, distinguishing genuine biological signal from procedural artefact becomes critically important. A slight elevation in cytokine concentration may represent true disease activity, therapeutic response, or simply ongoing release from incompletely removed inflammatory cells remaining within inadequately processed plasma.
Consequently, laboratory personnel frequently operate with awareness that operational precision directly influences scientific interpretability. The second or third spin therefore becomes part of a broader attempt to protect biological truth from procedural distortion.
Yet repeated centrifugation itself requires careful balance. Excessive centrifugal force may damage fragile biological structures. Over-processing may contribute to protein denaturation or mechanical stress. Different biomarkers demonstrate differing sensitivities to centrifugation conditions. Thus, repeated spinning is not universally beneficial under all circumstances but must be carefully calibrated according to analytical objectives, disease context, assay requirements, and specimen type.
This highlights another often overlooked aspect of laboratory science: optimisation is highly contextual.
Clinical laboratories continuously navigate competing priorities involving efficiency, sample stability, regulatory compliance, staffing limitations, assay requirements, and operational throughput. High-volume laboratories processing hundreds or thousands of specimens daily must maintain standardisation while simultaneously adapting to biological variability between samples. Scientific consistency therefore depends upon disciplined procedural systems capable of functioning reliably under operational pressure.
The emotional dimension of laboratory work is also rarely acknowledged publicly. Unlike physicians who interact directly with patients, laboratory personnel frequently operate without visible recognition despite handling materials directly connected to human illness, therapeutic uncertainty, and clinical outcomes. Every tube represents an individual patient participating in scientific investigation, often hoping experimental therapies may improve chronic disease conditions.
Within AERD clinical trials, this reality becomes particularly tangible. Many patients enrolled in inflammatory disease research have experienced years of respiratory distress, chronic sinus disease, repeated surgeries, medication dependency, and therapeutic frustration. Blood samples collected from these individuals are not abstract scientific materials detached from lived experience. They represent biological narratives of inflammation, treatment response, and disease burden.
The clinical trial laboratory therefore occupies an unusual position between operational science and human medicine. It exists simultaneously as a technical environment governed by protocols and as a translational space contributing to therapeutic advancement. Scientific precision within the laboratory ultimately serves broader clinical purposes extending far beyond the centrifuge itself.
As biomedical research increasingly advances toward precision medicine, personalised therapeutics, and biomarker-driven treatment systems, the strategic importance of laboratory optimisation will continue expanding. Advanced analytical technologies including multiplex cytokine profiling, genomic sequencing, proteomics, metabolomics, and artificial intelligence-assisted diagnostics all depend fundamentally upon the quality of biological inputs entering these systems.
No analytical platform, regardless of sophistication, can fully compensate for compromised sample integrity. (Lippi et al., 2011; Plebani, 2006)
For this reason, pre-analytical optimisation deserves greater recognition as a scientific discipline rather than merely an operational routine. Repeated centrifugation, large component adjustment, and plasma refinement strategies should be understood within this broader framework of preserving analytical reliability in increasingly sensitive biomedical environments.
The modern clinical trial laboratory is therefore not simply a place where blood is processed. It is a controlled scientific ecosystem responsible for protecting the integrity of biological information before interpretation even begins.
CHAPTER 4
THE SCIENCE OF CENTRIFUGATION AND LARGE COMPONENT ADJUSTMENT
Among the many instruments occupying the modern clinical laboratory, few appear as outwardly ordinary yet scientifically consequential as the centrifuge. Unlike advanced molecular analysers displaying complex computational interfaces or high-throughput sequencing platforms associated with cutting-edge biomedical innovation, the centrifuge often exists quietly within the operational background of laboratory workflows. Its purpose appears deceptively simple: to spin blood at controlled speeds in order to separate biological components according to density. Yet beneath this apparent simplicity lies a process deeply connected to the preservation of analytical integrity, biomarker reliability, and scientific reproducibility.
Within clinical trial laboratories, centrifugation is not merely a preparatory procedure preceding “real” analysis. It is itself a form of analytical intervention. The quality of centrifugation influences what downstream technologies are ultimately able to detect, quantify, interpret, or potentially miss entirely. Particularly within allergy and immunology research involving inflammatory disease states such as Aspirin-Exacerbated Respiratory Disease (AERD), the centrifugation process becomes central to maintaining the biological fidelity of collected specimens.
To understand why repeated spinning may enhance laboratory data quality, it is first necessary to understand the scientific principles underlying blood separation itself.
Blood is a heterogeneous biological suspension composed of cellular structures, proteins, lipids, electrolytes, inflammatory mediators, hormones, antibodies, metabolic products, and dissolved gases. Under normal physiological conditions, these components circulate dynamically throughout the vascular system in carefully regulated balance. However, once blood is collected into laboratory tubes and removed from the body, this equilibrium begins to change. Biological systems that were previously stabilised through physiological regulation become vulnerable to mechanical disruption, temperature shifts, metabolic continuation, and inflammatory activation.
Centrifugation attempts to stabilise this instability through physical separation.
The process relies upon centrifugal force generated through rapid rotational motion. When blood tubes spin within a centrifuge rotor, denser materials experience greater outward force relative to lighter components. Over time, this differential movement causes blood fractions to separate spatially according to mass and density characteristics.
Red blood cells, which possess relatively high density due to haemoglobin concentration and cellular mass, migrate toward the bottom of the collection tube. Plasma, being primarily liquid, remains at the upper portion of the tube. Between these layers forms the buffy coat, consisting largely of leukocytes and platelets.
While textbooks frequently present this separation as clean and definitive, laboratory reality is considerably more nuanced. Biological materials rarely separate perfectly after a single centrifugation cycle. Microscopic residual particulates often remain suspended within plasma even when visual separation appears acceptable to the naked eye. Platelets may persist in varying concentrations. Small fibrin fragments, cellular microdebris, lipid particles, and inflammatory residues may continue circulating within the plasma layer despite initial processing.
Within routine clinical chemistry, these residual materials may not always produce major analytical concern. However, within highly sensitive immunological assays or biomarker-driven clinical research, even subtle contamination may influence downstream measurements significantly.
The importance of plasma purity becomes increasingly evident in inflammatory disease studies where biomarker concentrations are often extremely low, highly dynamic, or biologically fragile. Cytokines, for example, may exist within picogram-per-millilitre concentrations. Small amounts of residual platelet activation or leukocyte contamination may artificially alter measurable inflammatory profiles. Consequently, what appears operationally insignificant may become scientifically substantial. (de Jager et al., 2009)
Repeated centrifugation emerges from this operational-scientific tension.
The first centrifugation cycle primarily accomplishes gross separation. It isolates major blood fractions sufficiently for many standard applications. However, secondary or tertiary spins may further refine plasma quality by progressively reducing remaining particulates and residual cellular materials. Large component adjustment therefore refers not simply to repeated spinning as repetition for its own sake but rather to iterative refinement of biological separation.
In many clinical trial laboratories, personnel begin recognising subtle visual differences between singly spun and repeatedly spun plasma over time through practical experience. Following initial centrifugation, plasma may retain slight turbidity, faint cloudiness, microscopic particulate traces, or platelet suspension that become more apparent under careful observation. Subsequent centrifugation frequently produces plasma that appears optically cleaner and more uniform.
Yet the true significance of this refinement extends beyond appearance alone.
Repeated spinning may reduce residual platelet concentrations substantially. This matters because platelets are biologically active inflammatory participants rather than passive coagulation fragments. Platelets release cytokines, chemokines, growth factors, and inflammatory mediators capable of altering plasma composition during storage and handling. In inflammatory diseases such as AERD, where platelet-leukocyte interactions may already contribute to disease mechanisms, residual platelet contamination may complicate biomarker interpretation further.
Similarly, incompletely removed leukocytes may continue releasing intracellular substances after collection. White blood cells remain metabolically active for periods following venepuncture. Cytokine release, enzymatic activity, and inflammatory signalling may continue outside the body if samples are not adequately processed. Repeated centrifugation seeks to minimise these post-collection biological alterations by improving removal efficiency.
The scientific logic underpinning repeated centrifugation therefore aligns closely with the broader concept of pre-analytical control.
Pre-analytical variability refers to any alteration in sample composition occurring before formal laboratory analysis begins. This includes variability introduced through collection technique, transport conditions, timing inconsistencies, temperature fluctuations, haemolysis, clot formation, centrifugation conditions, aliquoting errors, or storage instability. Numerous studies across laboratory medicine have demonstrated that pre-analytical variability may contribute substantially to overall laboratory error rates. (Lippi et al., 2011; Plebani, 2006)
Importantly, pre-analytical variability is especially problematic because it often remains invisible during downstream analysis. Analytical instruments may produce highly precise measurements from biologically compromised samples without recognising that the original specimen integrity has already been altered. Sophisticated assay platforms cannot distinguish perfectly between genuine physiological signals and artefacts introduced during sample preparation. (Lippi et al., 2011; Yin et al., 2013)
Consequently, laboratory optimisation increasingly focuses not only upon analytical instrumentation but also upon upstream procedural refinement.
Within clinical trial environments, this issue becomes even more critical because datasets generated from biological samples may influence pharmaceutical development, regulatory approval pathways, and future therapeutic strategies. Clinical trials depend upon consistency. Variability originating from laboratory handling rather than patient biology introduces interpretational uncertainty into research findings.
The challenge is particularly significant in translational immunology where inflammatory biomarkers often demonstrate narrow dynamic ranges and substantial biological sensitivity. Small deviations in processing conditions may disproportionately affect measured outcomes.
Consider cytokine analysis within AERD research. Cytokines function as signalling proteins coordinating inflammatory communication between immune cells. Their concentrations may fluctuate rapidly depending upon disease state, medication exposure, stress responses, infection, allergen interaction, or therapeutic intervention. Many cytokines also demonstrate short biological half-lives and vulnerability to degradation or artificial release during improper handling.
If residual inflammatory cells remain within inadequately processed plasma, cytokine concentrations measured hours later may no longer reflect true in vivo patient physiology. Instead, measured values may partly represent ongoing ex vivo cellular activity occurring after collection. The distinction between patient biology and procedural artefact becomes blurred. (de Jager et al., 2009; Aziz et al., 1999)
Repeated centrifugation attempts to preserve the original biological state of the sample more accurately by minimising these confounding influences.
However, repeated spinning itself requires scientific balance and procedural discipline.
Excessive centrifugation may introduce new forms of sample stress. High centrifugal forces can potentially damage fragile cellular structures or alter protein stability. Over-processing may increase haemolysis risk or contribute mechanical disruption affecting certain analytes. Therefore, large component adjustment should not be interpreted as indiscriminate repetition but rather as controlled optimisation guided by analytical objectives and specimen requirements.
Different laboratories may adopt varying centrifugation protocols depending upon assay sensitivity, sample type, disease context, and regulatory frameworks. Variables commonly adjusted include:
- centrifugation speed (RPM or relative centrifugal force),
- spin duration,
- rotor type,
- braking intensity,
- acceleration settings,
- temperature conditions,
- plasma transfer technique,
- and timing between sequential spins.
Even small changes within these parameters may influence plasma quality outcomes.
Temperature control during centrifugation also carries substantial importance. Certain biomarkers demonstrate temperature sensitivity and may degrade under inappropriate thermal conditions. Refrigerated centrifugation helps preserve stability for temperature-sensitive analytes while reducing ongoing metabolic activity. However, not all assays require identical handling conditions, further reinforcing the complexity of laboratory optimisation.
Operationally, repeated centrifugation introduces additional workload demands within already time-sensitive laboratory systems. Secondary and tertiary spins require more handling time, greater equipment availability, additional monitoring, and increased procedural coordination. High-throughput clinical laboratories processing large specimen volumes must continuously balance optimisation goals against workflow efficiency constraints.
This operational tension reflects a broader issue within laboratory medicine: the constant negotiation between ideal scientific conditions and practical clinical realities.
In theory, every sample could undergo highly customised optimisation protocols designed specifically for maximal analytical purity. In practice, laboratories operate within constraints involving staffing, instrumentation capacity, turnaround times, freezer space, regulatory compliance, and clinical deadlines. Consequently, laboratory science frequently involves strategic compromise while attempting to preserve acceptable analytical integrity.
Within clinical trial settings, however, the threshold for acceptable variability is often lower because research-grade samples may support highly sensitive investigational endpoints. Biomarker precision becomes more important when datasets contribute directly to evaluating therapeutic efficacy or mechanistic understanding.
Large component adjustment through repeated spinning therefore becomes especially valuable in contexts where biomarker reliability carries substantial translational importance.
Another often overlooked aspect of centrifugation science involves visual interpretation by experienced laboratory personnel. Although laboratory protocols emphasise standardisation, experienced technicians frequently develop observational sensitivity toward subtle indicators of sample quality. Slight plasma haze, unusual colouration, delayed separation patterns, fibrin traces, or platelet suspension may become recognisable signs suggesting additional processing may improve sample integrity.
This experiential knowledge reflects the deeply human dimension of laboratory science.
Laboratory expertise is not derived solely from written protocols but also from repeated exposure to biological variability across thousands of samples processed over time. Personnel begin recognising patterns not always fully captured within standard operating procedures. The ability to identify when a specimen may benefit from additional centrifugation often develops through accumulated operational experience.
Yet despite the importance of this expertise, laboratory work remains comparatively invisible within broader healthcare narratives.
Patients rarely witness the operational complexity occurring after blood collection. Pharmaceutical publications seldom emphasise the labour intensity underlying biomarker preparation. Scientific papers frequently focus on statistical outcomes while dedicating minimal discussion to the nuanced realities of pre-analytical optimisation. Nevertheless, the reliability of many published findings depends heavily upon these hidden operational processes.
The centrifuge therefore symbolises something larger within clinical research ecosystems.
It represents the interface between raw biological complexity and interpretable scientific data.
Before computational modelling, before biomarker quantification, before statistical analysis, and before therapeutic interpretation, blood must first undergo transformation into analytically stable biological material. Repeated spinning becomes part of this transformation process. The second spin is not merely mechanical repetition. It is an attempt to reduce uncertainty. The third spin is not procedural excess. It is an effort to preserve biological clarity within systems vulnerable to variability.
Within allergy and immunology research involving AERD, where inflammatory pathways are intricate and biomarker interpretation demands high sensitivity, these operational refinements become especially meaningful.
Ultimately, centrifugation should not be understood merely as laboratory preparation. It is an active scientific process shaping the quality of evidence from which modern biomedical understanding emerges.
CHAPTER 5
REPEATED SPINNING, PLASMA PURITY, AND BIOMARKER PRESERVATION IN AERD RESEARCH
Within the operational environment of a clinical trial laboratory, few moments are as deceptively important as the period immediately following centrifugation. At first glance, the separation of blood into distinct visible layers appears to signal procedural completion. Red blood cells settle beneath the plasma, the buffy coat becomes faintly visible, and the specimen appears technically processed. However, for laboratories involved in advanced immunological and inflammatory disease research, this moment frequently marks not the end of preparation but the beginning of refinement.
The concept of repeated spinning emerges precisely from this understanding: that visible separation does not necessarily guarantee analytical purity.
In highly sensitive allergy and immunology studies, particularly those involving Aspirin-Exacerbated Respiratory Disease (AERD), the biological reliability of plasma extends beyond basic component isolation. The objective is not merely to obtain plasma but to obtain plasma sufficiently refined to preserve subtle immunological signals while minimising procedural interference. This distinction fundamentally reshapes the role of centrifugation within clinical research environments.
The importance of plasma purity becomes clearer when considering the biological complexity of inflammatory diseases. AERD is not a condition driven by a single pathway or isolated biomarker. It represents a dynamic inflammatory network involving eosinophilic activation, mast cell signalling, leukotriene dysregulation, platelet interactions, chronic respiratory inflammation, and altered arachidonic acid metabolism. These pathways interact continuously and produce biomarker environments characterised by fluctuation, sensitivity, and biological instability.
Consequently, many analytes measured within AERD research exist under conditions highly vulnerable to pre-analytical disruption.
Inflammatory biomarkers are particularly susceptible because immune cells remain biologically active even after blood collection. Unlike static chemical compounds, living cellular systems continue responding to environmental conditions outside the body. White blood cells may continue secreting cytokines. Platelets may become activated through mechanical handling. Coagulation-related pathways may remain partially active. Protein degradation may begin progressively depending upon temperature exposure and processing delays.
The blood sample therefore exists in a transitional biological state following collection. It no longer benefits from physiological regulation within the body, yet many biological processes remain temporarily active. The role of the laboratory is to stabilise this instability as rapidly and consistently as possible.
Repeated centrifugation functions as one method of achieving this stabilisation.
Following initial spinning, plasma may still contain microscopic residual elements not fully removed through single-cycle separation. These include platelets, leukocyte fragments, fibrin residues, lipid particles, cellular microdebris, and other suspended materials capable of interfering with downstream analysis. Although such contaminants may exist at concentrations visually undetectable to the naked eye, their presence may still influence highly sensitive immunological assays.
This becomes particularly important in studies involving cytokines and inflammatory mediators.
Cytokines are among the most analytically delicate biomarkers within immunology research. They function as molecular communication signals coordinating immune responses between cells. Their concentrations may fluctuate rapidly, often existing within extremely low measurable ranges. Small procedural inconsistencies may therefore alter cytokine measurements disproportionately relative to their baseline concentrations.
Residual platelets represent one of the major sources of potential analytical interference in this context. Historically associated primarily with coagulation, platelets are now increasingly recognised as active immunological participants contributing to inflammation, immune modulation, and disease pathogenesis. Within AERD specifically, platelet-leukocyte interactions have attracted growing scientific attention due to their role in leukotriene overproduction and inflammatory amplification. (Semple et al., 2011; Gros et al., 2014)
When residual platelets remain suspended within plasma following incomplete centrifugation, they may continue releasing inflammatory mediators during storage or handling. Consequently, measured cytokine or inflammatory marker concentrations may partially reflect ex vivo platelet activity rather than true patient physiology at the moment of collection.
Repeated spinning attempts to minimise this discrepancy.
The second centrifugation cycle frequently targets platelet reduction specifically. After transferring plasma from the initial tube into a secondary processing container, laboratories may perform additional centrifugation under carefully controlled conditions to remove residual suspended platelets and particulates more effectively. In some protocols, tertiary spins may further enhance plasma refinement for particularly sensitive downstream applications.
This progressive refinement process contributes to what many laboratory scientists informally describe as “clean plasma.” However, cleanliness within this context refers not simply to visual appearance but to biological reduction of interfering materials capable of distorting analytical outcomes.
The difference between standard plasma and highly refined plasma may become especially relevant when using advanced analytical platforms such as multiplex cytokine assays, flow cytometry, proteomic analysis, mass spectrometry, or biomarker-driven translational studies. These technologies possess increasingly high sensitivity capable of detecting minute biological differences. Yet increased analytical sensitivity simultaneously increases vulnerability to pre-analytical contamination.
This creates an important paradox within modern biomedical science.
As analytical technologies become more advanced, the importance of basic laboratory handling often increases rather than decreases.
Sophisticated instrumentation cannot fully compensate for compromised specimen quality. In fact, highly sensitive assays may magnify the consequences of poor pre-analytical preparation because they detect subtle variations arising not only from disease biology but also from handling inconsistencies. The reliability of advanced biomedical technologies therefore remains fundamentally dependent upon the quality of biological inputs entering these systems.
Repeated spinning should therefore be understood within the broader framework of biomarker preservation rather than mere procedural repetition.
Biomarker preservation refers to maintaining the biological state of the specimen as close as possible to its original physiological condition at the time of collection. The objective is not to alter the sample artificially but to prevent unwanted post-collection changes capable of obscuring meaningful biological information.
This distinction is critically important within clinical trial environments because therapeutic conclusions may depend upon relatively small measurable differences between treatment groups. A modest reduction in inflammatory cytokine levels following investigational therapy may represent meaningful therapeutic response. However, if biomarker variability arises partly from inconsistent plasma processing rather than actual biological effects, scientific interpretation becomes more uncertain.
Clinical trials therefore rely heavily upon procedural standardisation to minimise avoidable variability.
Standard operating procedures within research laboratories often specify precise centrifugation parameters including: (Tuck et al., 2009; Rai et al., 2005)
- relative centrifugal force,
- revolutions per minute,
- spin duration,
- acceleration profiles,
- deceleration settings,
- temperature conditions,
- plasma transfer techniques,
- aliquoting procedures,
- and acceptable processing timelines.
These protocols exist because pre-analytical variability represents one of the largest sources of hidden laboratory inconsistency. (Lippi et al., 2011; Yin et al., 2013)
However, operational reality introduces additional complexity beyond written procedures alone.
Not all blood samples behave identically during centrifugation. Biological variability between patients significantly affects specimen characteristics. Some samples separate rapidly and cleanly. Others demonstrate delayed separation, increased lipid content, fibrin formation, clotting tendencies, haemolysis susceptibility, or persistent particulate suspension despite standard processing.
Inflammatory disease states themselves may alter blood properties. Elevated inflammatory proteins, altered coagulation pathways, medication effects, chronic steroid exposure, or immune activation may all influence centrifugation behaviour. Consequently, laboratory personnel frequently develop procedural awareness extending beyond strict protocol memorisation.
Experienced laboratory scientists often recognise subtle indicators suggesting that additional spinning may improve specimen quality. Slight plasma turbidity, faint platelet haze, microfibrin traces, or incomplete separation patterns may become operational cues supporting repeated centrifugation decisions. This form of expertise develops gradually through repeated exposure to biological variability across thousands of specimens.
The human observational dimension of laboratory science is therefore more important than many outside the field realise.
Although clinical laboratories emphasise automation and standardisation, scientific reliability still depends heavily upon disciplined human judgement. Personnel must continuously interpret sample conditions, prioritise workflows, monitor equipment behaviour, and maintain procedural consistency under operational pressure.
This becomes especially challenging within busy clinical trial laboratories where large numbers of time-sensitive specimens arrive simultaneously according to patient scheduling and therapeutic protocols. Blood samples frequently require processing within narrow stability windows. Delays may compromise biomarker integrity. Equipment availability must be coordinated efficiently. Freezer preparation, aliquoting, documentation, and chain-of-custody systems must all function synchronously.
Repeated centrifugation therefore introduces both scientific advantages and operational burdens.
Additional spins require more processing time, greater equipment utilisation, increased handling steps, and additional opportunities for procedural error if not carefully managed. Laboratories must balance optimisation goals against practical throughput limitations and staffing realities. Scientific idealism must coexist with operational feasibility.
Nevertheless, within highly sensitive immunological research, the benefits of refined plasma preparation often justify these additional efforts.
Another important consideration involves long-term specimen storage.
Many clinical trial samples are not analysed immediately following collection. Plasma may be aliquoted and stored at ultra-low temperatures for weeks, months, or even years before downstream biomarker analysis occurs. During long-term storage, residual cellular materials remaining within inadequately processed plasma may continue influencing specimen integrity through freeze-thaw instability, protein degradation, or ongoing release of intracellular substances prior to complete freezing.
Cleaner plasma generated through repeated spinning may therefore contribute not only to immediate assay quality but also to long-term specimen stability.
This becomes increasingly important in longitudinal clinical studies where stored biospecimens may later support retrospective biomarker investigations, translational research, or future analytical technologies not yet available during initial sample collection. The quality of today’s laboratory preparation may influence tomorrow’s scientific discoveries.
Within AERD research specifically, this carries particular significance because the disease remains incompletely understood despite growing scientific interest. Biomarker exploration continues evolving rapidly. Stored plasma specimens collected under carefully controlled conditions may eventually contribute to identifying new inflammatory pathways, therapeutic targets, or disease phenotypes.
The laboratory therefore participates not only in present analysis but also in future scientific possibility.
Repeated spinning also intersects with broader themes within precision medicine.
Modern medicine increasingly seeks to classify diseases according to molecular characteristics, inflammatory signatures, and biomarker-defined subtypes rather than broad symptomatic categories alone. Precision medicine depends fundamentally upon the ability to detect subtle biological differences reliably. As biomarker-driven medicine expands, the importance of refined specimen preparation correspondingly increases.
The future of translational immunology will likely involve increasingly sensitive analytical systems capable of evaluating highly specific inflammatory profiles. Artificial intelligence-assisted biomarker interpretation, proteomic mapping, metabolomic analysis, and personalised therapeutic targeting will all depend heavily upon specimen integrity at the pre-analytical stage.
In this context, large component adjustment through repeated centrifugation should not be viewed as an outdated manual refinement technique overshadowed by technological advancement. On the contrary, it represents a foundational practice supporting the reliability of increasingly sophisticated biomedical systems.
The second spin ultimately symbolises something larger than procedural optimisation alone.
It reflects the recognition that scientific accuracy is cumulative. Reliable biomedical knowledge does not emerge solely from advanced instrumentation or statistical sophistication. It begins earlier, within operational decisions designed to preserve biological truth before analysis even starts.
Within the quiet environment of the clinical trial laboratory, repeated spinning becomes part of a larger scientific philosophy: that even the smallest procedural refinements may influence the quality of evidence upon which future medicine is built.
CHAPTER 6
PROTOCOL IN PRACTICE: DOUBLE AND TRIPLE SPIN METHODOLOGY IN CLINICAL TRIAL BLOOD PROCESSING
In biomedical research, scientific error is often imagined as something dramatic and immediately recognisable. People envision malfunctioning analytical instruments, corrupted datasets, failed experiments, or obvious procedural mistakes capable of invalidating results instantly. However, within clinical laboratory science, many of the most consequential forms of variability emerge quietly, gradually, and almost invisibly through small inconsistencies accumulating during routine operational workflows. These inconsistencies rarely announce themselves openly. Instead, they become embedded subtly within datasets, biomarker profiles, inflammatory measurements, and statistical outputs until they are no longer easily distinguishable from genuine biological variation.
This hidden domain of scientific inconsistency is commonly referred to as pre-analytical variability.
Pre-analytical variability encompasses every alteration affecting specimen integrity before formal laboratory analysis begins. It includes variables introduced during patient preparation, blood collection, transport, centrifugation, plasma separation, aliquoting, storage, handling, documentation, and timing coordination. Although downstream analytical technologies often receive the greatest scientific attention, extensive evidence within laboratory medicine suggests that a substantial proportion of laboratory variability originates during these earlier operational stages. (Lippi et al., 2011; Plebani, 2006)
In many respects, pre-analytical variability represents one of the most underestimated challenges within modern clinical research.
This underestimation exists partly because pre-analytical inconsistencies are difficult to detect directly once samples enter analytical systems. Instruments process the biological material they receive without fully recognising the procedural history that shaped specimen quality beforehand. If cytokine concentrations shift due to residual platelet activation during transport, or if inflammatory markers degrade because of delayed centrifugation, downstream assays may still generate precise numerical outputs despite compromised biological integrity. The resulting data may appear technically accurate while no longer representing the original physiological state of the patient at the moment of collection.
This distinction between analytical precision and biological accuracy is critically important.
A laboratory instrument may measure a biomarker with extraordinary technical precision while simultaneously analysing a specimen that has already undergone biological alteration during handling. Precision alone therefore does not guarantee validity. The reliability of biomedical interpretation depends not only upon how accurately instruments measure samples but also upon whether those samples still preserve meaningful physiological information.
Within allergy and immunology research involving diseases such as Aspirin-Exacerbated Respiratory Disease (AERD), this issue becomes particularly significant because inflammatory biomarkers are highly sensitive to procedural conditions. Cytokines, leukotrienes, eosinophilic markers, chemokines, and inflammatory proteins often exist within biologically dynamic environments where even small disturbances may influence measurable concentrations.
The laboratory therefore functions as a protective environment attempting to stabilise inherently unstable biological systems.
Yet despite extensive procedural standardisation, the human factor remains deeply embedded within laboratory operations.
This reality is often overlooked in public discussions of scientific research. Laboratories are commonly imagined as fully controlled technological environments governed entirely by automation and protocol. However, clinical laboratory science remains fundamentally dependent upon human coordination, observation, timing, and judgement. Human beings collect the blood, label the tubes, operate the centrifuges, transfer the plasma, aliquot the specimens, monitor freezer conditions, document processing timelines, and manage workflow prioritisation under operational pressure.
Consequently, the quality of laboratory data depends not only upon instrumentation but also upon the consistency of human operational behaviour.
This does not imply negligence or incompetence. On the contrary, laboratory professionals operate under highly disciplined procedural systems specifically designed to reduce avoidable variability. Nevertheless, biological processing occurs within real-world environments involving time constraints, staffing limitations, equipment demands, scheduling pressures, and unpredictable specimen conditions. Variability therefore becomes something laboratories continuously attempt to manage rather than eliminate entirely.
One of the earliest sources of pre-analytical variability begins even before blood enters the collection tube.
Patient physiology itself fluctuates continuously according to numerous biological and environmental factors. Circadian rhythms influence hormone levels and inflammatory signalling. Medication exposure alters metabolic pathways. Fasting status affects lipid concentrations and glucose regulation. Stress responses may influence cortisol and cytokine activity. Hydration status alters plasma volume. Physical activity, infection, sleep patterns, smoking exposure, and allergen contact may all shape measurable biomarker profiles prior to collection.
In inflammatory diseases such as AERD, these fluctuations may become even more pronounced because immune activity itself is inherently dynamic.
Consequently, clinical trial protocols often attempt to standardise patient preparation conditions carefully. Blood collection may occur at fixed times relative to medication administration or therapeutic intervention. Patients may be instructed regarding fasting requirements or activity restrictions. Collection windows may be tightly controlled to reduce temporal variability between specimens.
Yet despite these efforts, biological variability can never be completely eliminated because human physiology itself is not static.
Following venepuncture, additional procedural variables emerge immediately.
The collection process may appear routine, yet numerous subtle factors influence specimen quality at this stage alone. Needle gauge affects shear stress on blood cells. Difficult venous access may increase haemolysis risk. Prolonged tourniquet application may alter local biochemical concentrations. Forceful aspiration may damage fragile cellular structures. Delayed tube inversion may contribute to clot formation.
Even the order in which collection tubes are filled carries scientific importance because additive carryover between tubes may affect downstream assays.
Once blood enters the collection tube, the specimen enters a transitional biological state where laboratory timing becomes increasingly important. Cellular metabolism continues temporarily outside the body. Platelets remain responsive to mechanical stimulation. Leukocytes may continue releasing inflammatory mediators. Coagulation pathways may remain partially active depending upon anticoagulant conditions.
The interval between collection and centrifugation therefore becomes one of the most critical phases within specimen handling. (Flower et al., 2000; Lippi et al., 2011)
Delays during this period may substantially alter sample composition. Cytokine concentrations may shift. Glucose levels may decline due to ongoing cellular metabolism. Potassium concentrations may rise through cellular leakage. Inflammatory proteins may degrade. Residual clotting activity may generate fibrin interference.
For highly sensitive immunological assays, even relatively short delays may become analytically relevant.
This is why many clinical trial laboratories operate under strict processing timelines specifying maximum allowable intervals between collection and centrifugation. Samples may require immediate transport from clinical sites to processing laboratories. Dedicated couriers, timed workflows, and priority handling systems are frequently implemented to minimise instability during this vulnerable period.
However, operational reality introduces practical challenges continuously.
Clinical trial laboratories often process large numbers of specimens arriving simultaneously according to patient schedules. Unexpected delays may occur due to equipment availability, staffing demands, specimen volume surges, or transport logistics. Laboratories must therefore maintain procedural discipline while adapting dynamically to real-time workflow conditions.
The centrifugation stage itself introduces additional opportunities for variability if not carefully controlled.
Centrifugation parameters such as relative centrifugal force, spin duration, acceleration rate, braking intensity, rotor balance, and temperature conditions all influence separation outcomes. Even when protocols specify standard settings, small inconsistencies in implementation may affect plasma quality subtly.
Improper balancing within centrifuge rotors may generate uneven separation. Excessive braking may disturb separated layers during deceleration. Insufficient centrifugal force may leave residual platelet contamination. Overly aggressive force may contribute to haemolysis or protein disruption.
Repeated spinning strategies attempt partly to reduce some of these inconsistencies by further refining plasma separation after initial processing.
However, plasma transfer between sequential spins introduces another highly delicate operational phase.
The act of aspirating plasma from above the buffy coat requires precision and experience. If pipette tips approach the buffy coat too closely, leukocyte contamination may occur. Excessively cautious transfer may reduce plasma yield unnecessarily. Microdisturbances during handling may resuspend particulates into otherwise refined plasma.
This stage highlights the important relationship between procedural standardisation and human dexterity within laboratory work.
Certain aspects of laboratory science cannot be fully automated because they involve nuanced biological judgement developed through operational experience. Skilled laboratory personnel often develop strong visual and tactile familiarity with specimen behaviour. They begin recognising subtle indicators of haemolysis, incomplete separation, platelet haze, fibrin contamination, or abnormal plasma characteristics not always fully described within procedural manuals.
This experiential expertise represents a significant yet often invisible scientific asset within laboratory systems.
Importantly, emotional and cognitive factors also influence laboratory environments in ways rarely discussed openly within scientific literature.
Clinical trial laboratories frequently operate under high-pressure conditions involving strict regulatory oversight, time-sensitive specimens, extensive documentation requirements, and large operational workloads. Personnel may process hundreds of samples daily while maintaining concentration across repetitive yet highly consequential procedures.
Fatigue, workflow congestion, interruptions, multitasking demands, and cognitive overload may all subtly affect operational consistency even within highly disciplined environments.
This does not imply carelessness. Rather, it reflects the reality that laboratory systems remain human systems despite technological advancement.
The psychological invisibility of laboratory work within broader healthcare structures may also contribute indirectly to operational strain. Unlike physicians or nurses who receive visible patient interaction and public recognition, laboratory professionals frequently work behind closed operational environments with minimal public awareness of their contributions. Yet the reliability of medical decisions often depends heavily upon their precision.
Every therapeutic conclusion emerging from clinical research ultimately rests upon chains of laboratory handling extending back to the earliest moments of specimen preparation.
Within AERD clinical trials, this reality carries particular significance because therapeutic investigations increasingly rely upon biomarker-driven interpretation. Biological therapies targeting inflammatory pathways require accurate assessment of cytokine activity, eosinophilic behaviour, leukotriene modulation, and immunological response patterns. Subtle biomarker shifts may influence conclusions regarding treatment efficacy, dosing strategies, or patient stratification.
Consequently, hidden pre-analytical variability may influence translational medicine outcomes more than many outside laboratory science realise.
Another major source of variability involves freeze-thaw cycles during long-term specimen storage.
Many clinical trial samples undergo storage before analysis occurs. Biomarker stability during storage depends upon temperature integrity, aliquot design, storage duration, freezer consistency, and minimisation of repeated thawing events. Certain cytokines degrade after repeated freeze-thaw exposure. Proteins may denature. Residual cellular materials may release intracellular contents during incomplete freezing or thawing instability. (Flower et al., 2000; de Jager et al., 2009)
Repeated spinning before storage may improve long-term stability partly by reducing residual cellular contamination capable of altering plasma composition during storage periods. (Tuck et al., 2009; de Jager et al., 2009)
This illustrates an important principle underlying laboratory optimisation: procedural refinements frequently generate cumulative benefits across multiple downstream stages.
Cleaner plasma improves not only immediate assay reliability but also storage stability, reproducibility, inter-laboratory consistency, and future analytical compatibility.
As biomedical science advances toward increasingly sensitive analytical systems, the consequences of pre-analytical variability may become even more significant rather than less.
Artificial intelligence-assisted diagnostics, proteomics, metabolomics, precision immunology, and ultra-sensitive biomarker platforms all depend fundamentally upon high-quality biological inputs. Sophisticated computational systems cannot fully correct for compromised specimen integrity introduced during earlier operational stages.
The future of precision medicine therefore depends partly upon recognising the strategic importance of pre-analytical control.
Within this broader scientific landscape, repeated centrifugation and large component adjustment represent more than technical refinements alone. They reflect a deeper scientific philosophy acknowledging that reliable knowledge emerges through cumulative operational precision. Biomedical truth is not produced exclusively by advanced analytical technologies. It is preserved gradually through disciplined handling of biological materials vulnerable to instability at every stage of their journey through the laboratory.
The invisible work occurring before analysis often determines the reliability of everything that follows.
While theoretical discussions regarding plasma refinement and pre-analytical optimisation are important, translational medicine ultimately depends upon reproducible operational methodology. Clinical laboratories require not only conceptual frameworks but also practical systems capable of generating high-integrity biospecimens under real-world clinical trial conditions.
This chapter outlines a proposed double-spin and triple-spin centrifugation framework designed for allergy and immunology research involving inflammatory biomarker analysis, particularly within studies involving Aspirin-Exacerbated Respiratory Disease (AERD). The protocol should be adapted according to institutional requirements, assay sensitivity, centrifuge specifications, biomarker stability characteristics, and regulatory frameworks.
Sample Collection
Recommended Collection Tubes
| Tube Type | Anticoagulant | Primary Use |
| EDTA | EDTA | Cytokines, inflammatory markers |
| Sodium Citrate | Sodium Citrate | Coagulation-related investigations |
| SST (Serum Separator) | None (serum) | Serum-specific assays |
| Lithium Heparin | Heparin | Some metabolite assays |
Pre-Collection Conditions
Where clinically feasible, the following should be standardised before specimen collection:
- fasting status should be documented and controlled;
- collection timing should be fixed relative to medication administration;
- inflammatory status and any acute infection should be recorded;
- recent allergen exposure should be noted;
- steroid medication history should be documented.
Immediate Post-Collection Handling
- Invert tubes gently 8–10 times immediately after collection;
- avoid vigorous shaking to minimise haemolysis risk;
- maintain specimens upright during transport;
- minimise transport delays to preserve biomarker stability;
- begin processing within 30–60 minutes of collection for sensitive inflammatory analytes.
Centrifugation Protocol Summary
The following table summarises recommended parameters across all three centrifugation stages:
| Parameter | Primary Spin | Secondary Spin | Tertiary Spin* |
| RCF | 1,500–2,000 × g | 2,000–3,000 × g | 3,000–5,000 × g |
| Duration | 10–15 min | 10 min | 10 min |
| Temperature | 4°C | 4°C | 4°C |
| Brake | Low / controlled | Low / controlled | Minimal |
| Objective | Gross separation | Platelet reduction | Microparticle removal |
* Tertiary centrifugation is optional and reserved for ultra-sensitive analytical applications only.
Primary Centrifugation
Objective
Gross separation of major blood components into red blood cell fraction, buffy coat layer, and plasma.
Procedure
- Place labelled tubes in calibrated refrigerated centrifuge;
- Balance rotor load symmetrically;
- Set parameters: 1,500–2,000 × g, 10–15 minutes, 4°C;
- Select low brake / controlled deceleration to preserve layer integrity;
- Following completion, inspect separation visually before proceeding.
Expected Separation
- Red blood cells settle at the base of the tube;
- buffy coat forms a thin intermediate layer containing leukocytes and platelets;
- plasma occupies the upper fraction.
Plasma Transfer
Critical Handling Considerations
Plasma transfer represents one of the most sensitive procedural stages. Disturbance of the buffy coat during aspiration is the most frequent source of leukocyte and platelet contamination in this phase. Residual leukocyte contamination may significantly affect cytokine stability and inflammatory measurements.
Recommended Practice
- Use sterile low-retention pipette tips;
- aspirate plasma slowly using consistent negative pressure;
- maintain clear visual separation from the buffy coat interface;
- stop aspiration at least 5–10 mm above the buffy coat surface;
- transfer plasma into a clean labelled secondary tube immediately;
- document transfer time.
Secondary Centrifugation (Double Spin)
Objective
Progressive reduction of residual platelets, leukocyte fragments, fibrin traces, and microscopic particulates remaining following primary centrifugation.
Scientific Rationale
The second spin is particularly important for the following analytical applications:
- cytokine profiling using multiplex or singleplex platforms;
- proteomic analysis;
- ELISA-based inflammatory mediator quantification;
- flow cytometry involving soluble mediators;
- ultra-sensitive biomarker detection.
Residual platelets within singly centrifuged plasma remain biologically active and may release inflammatory mediators during storage, artificially altering measured concentrations of cytokines, chemokines, and related analytes.
Procedure
- Centrifuge transferred plasma at 2,000–3,000 × g for 10 minutes at 4°C;
- Apply low braking during deceleration;
- Inspect plasma visually — clarity should be improved compared to post-primary spin;
- Transfer refined plasma carefully to labelled cryovials;
- Proceed to aliquoting immediately.
Tertiary Centrifugation (Triple Spin — Optional)
Recommended Contexts
Triple spinning is not required for standard clinical laboratory workflows. It may be appropriate in the following specialised contexts:
- extracellular vesicle (EV) analysis;
- advanced proteomics requiring microparticle-free plasma;
- platelet-sensitive bioassays;
- ultra-low abundance cytokine measurements;
- AI-driven biomarker profiling platforms;
- precision immunology research applications.
Important Caution
Over-processing risks must be actively monitored when performing tertiary centrifugation.
Excessive centrifugal force may alter fragile proteins, increase haemolysis risk, damage extracellular structures, or introduce mechanical stress artefacts. Tertiary spinning should only be performed when analytically justified.
Aliquoting and Storage
Aliquoting Strategy
Plasma should be aliquoted immediately following final centrifugation. Aliquot volume should be designed to match anticipated assay requirements, minimising unnecessary thaw events.
- Recommended aliquot volume: 200–500 µL per cryovial;
- number of aliquots: determined by study protocol requirements;
- label cryovials with patient ID, visit number, collection date, and aliquot number.
Recommended Storage Conditions
- Short-term (under 30 days): −20°C;
- long-term (over 30 days): −80°C;
- ultra-sensitive biomarker applications: monitored ultra-low temperature systems with alarm infrastructure.
Freeze-Thaw Considerations
- Each freeze-thaw cycle introduces molecular stress;
- certain inflammatory cytokines degrade substantially after repeated thawing;
- multiple freeze-thaw events should be avoided through appropriate aliquot design;
- thawing should occur at 4°C to reduce thermal stress.
Quality Control Checkpoints
Visual Inspection Criteria
The following specimen characteristics should be assessed and documented at each stage:
| Finding | Possible Cause | Action |
| Haemolysis (pink/red plasma) | Rough handling, wrong needle gauge | Document, notify, consider repeat |
| Persistent turbidity after spin 1 | High lipid content, incomplete clotting | Proceed to second spin; document |
| Platelet haze after spin 2 | Insufficient RCF | Consider tertiary spin; document |
| Fibrin strands | Incomplete clotting (serum tubes) | Extend clotting time; record |
| Very low plasma yield | Clot formation in EDTA tube | Document, assess for rejection |
Documentation Requirements
The following must be recorded for every specimen processed:
- collection time and collection site;
- primary and secondary centrifugation timestamps;
- operator identity at each stage;
- centrifuge equipment ID and rotor used;
- visual inspection findings;
- deviations from protocol;
- aliquot volumes and cryovial locations;
- freezer assignment and storage timestamp.
Operational Significance
Biospecimen integrity is foundational to scientific reliability. Repeated centrifugation should not be understood merely as procedural repetition but as strategic refinement designed to preserve biological truth during the vulnerable transition between living physiology and measurable scientific evidence.
The protocol described within this chapter reflects the broader principle that pre-analytical laboratory handling is an active scientific intervention rather than passive technical preparation. Every stage — from venepuncture to freezer storage — shapes the quality of the biological information available for downstream analysis.
Within AERD clinical research, where inflammatory biomarkers reflect intricate and rapidly changing immunological environments, the discipline of repeated spinning may directly influence the reliability of therapeutic conclusions drawn from the dataset.
CHAPTER 7
PRE-ANALYTICAL VARIABILITY, HUMAN FACTORS, AND HIDDEN LABORATORY ERROR
In biomedical research, scientific error is often imagined as something dramatic and immediately recognisable. However, within clinical laboratory science, many of the most consequential forms of variability emerge quietly, gradually, and almost invisibly through small inconsistencies accumulating during routine operational workflows. This hidden domain of scientific inconsistency is commonly referred to as pre-analytical variability.
Pre-analytical variability encompasses every alteration affecting specimen integrity before formal laboratory analysis begins. It includes variables introduced during patient preparation, blood collection, transport, centrifugation, plasma separation, aliquoting, storage, handling, documentation, and timing coordination.
This underestimation exists partly because pre-analytical inconsistencies are difficult to detect directly once samples enter analytical systems. Instruments process the biological material they receive without fully recognising the procedural history that shaped specimen quality beforehand.
The interval between collection and centrifugation becomes one of the most critical phases within specimen handling. Delays during this period may substantially alter sample composition. Cytokine concentrations may shift. Inflammatory proteins may degrade. Residual clotting activity may generate fibrin interference. For highly sensitive immunological assays, even relatively short delays may become analytically relevant. (Flower et al., 2000; Aziz et al., 1999)
Another major source of variability involves freeze-thaw cycles during long-term specimen storage. Many clinical trial samples undergo storage before analysis occurs. Certain cytokines degrade after repeated freeze-thaw exposure. Repeated spinning before storage may improve long-term stability partly by reducing residual cellular contamination capable of altering plasma composition during storage periods. (Flower et al., 2000; de Jager et al., 2009)
CHAPTER 8
DATA ENHANCEMENT, SIGNAL PRESERVATION, AND SCIENTIFIC INTERPRETATION
Within modern biomedical research, the phrase “data enhancement” is often associated with computational systems, artificial intelligence, statistical modelling, algorithmic refinement, or high-dimensional analytical platforms capable of extracting increasingly sophisticated patterns from large datasets. However, within the clinical trial laboratory, data enhancement begins much earlier than computational analysis. It begins at the biological level itself, during the handling and preparation of specimens before numerical data has even been generated.
This distinction is critically important because biomedical data does not emerge spontaneously from machines alone. Data originates from biological materials that must first survive a complex chain of operational handling before analytical interpretation becomes possible. The reliability of downstream computational analysis therefore remains fundamentally dependent upon upstream biological integrity.
In this sense, the clinical laboratory functions as the first site of data construction within biomedical science.
Blood entering the laboratory is not yet “data” in the conventional statistical sense. It is biological potential. Within each specimen exists a dense network of physiological information waiting to be preserved, isolated, stabilised, and transformed into measurable analytical signals. The role of laboratory processing is to protect this information from distortion long enough for meaningful scientific interpretation to occur.
Repeated centrifugation and large component adjustment become significant within this framework because they operate as early-stage strategies for preserving biological signal quality.
The concept of signal preservation originates partly from systems theory, engineering, and analytical sciences where meaningful information must be separated from background interference or “noise.” Within laboratory medicine, biological signals refer to measurable biomarkers genuinely reflecting patient physiology, disease state, therapeutic response, or inflammatory behaviour. Noise refers to unwanted variability introduced through procedural artefacts, contamination, instability, degradation, or operational inconsistency.
The challenge within immunology research is that biological systems are inherently noisy even under ideal conditions.
Human physiology is extraordinarily dynamic. Cytokine concentrations fluctuate continuously. Immune cells respond rapidly to environmental stimuli. Platelets activate through mechanical stress. Hormonal cycles alter inflammatory pathways. Metabolic states shift according to time, stress, medication exposure, and disease activity. Consequently, the laboratory must distinguish between meaningful biological complexity and avoidable procedural distortion.
This distinction becomes especially difficult within inflammatory diseases such as Aspirin-Exacerbated Respiratory Disease (AERD).
AERD represents a chronic inflammatory condition characterised not only by respiratory symptoms but by widespread dysregulation across multiple immunological pathways. Leukotriene overproduction, eosinophilic inflammation, mast cell activation, platelet-leukocyte interactions, cytokine signalling abnormalities, and chronic airway inflammation collectively contribute to disease progression. Biomarkers associated with these pathways often exist within delicate physiological balances vulnerable to disruption during specimen handling.
The laboratory therefore becomes responsible for preserving these fragile biological relationships during processing.
Repeated spinning contributes to this preservation by progressively refining plasma purity and reducing sources of procedural interference. However, the scientific significance of this refinement extends beyond simple cleanliness. It influences how biological reality itself becomes represented within datasets.
This is a profound but often overlooked aspect of laboratory science: operational procedures shape scientific representation.
A biomarker value appearing within a spreadsheet, statistical model, or clinical trial report is not a direct mirror of biological reality untouched by laboratory intervention. Rather, it is the final outcome of multiple processing stages influencing what becomes measurable, detectable, amplified, suppressed, preserved, or potentially lost.
The laboratory therefore does not merely observe biology passively. It mediates the transition from biological state to scientific evidence.
This mediation becomes increasingly important as biomedical technologies grow more sensitive.
Modern immunological assays can detect analytes at extraordinarily low concentrations. Multiplex cytokine platforms simultaneously evaluate numerous inflammatory markers within small plasma volumes. Flow cytometry analyses cellular populations with remarkable precision. Proteomic technologies identify thousands of proteins within single specimens. Molecular assays detect subtle biological changes previously invisible to laboratory medicine.
Yet these technological advances create a paradox.
As analytical systems become more sensitive, they also become more vulnerable to pre-analytical disturbance.
Minor contamination previously considered insignificant may become detectable interference under highly sensitive analytical conditions. Residual platelets remaining after inadequate centrifugation may release sufficient inflammatory mediators to alter cytokine profiles measurably. Small amounts of haemolysis may distort downstream protein analysis. Slight delays in processing may influence unstable biomarkers disproportionately. (Lippi et al., 2011; Yin et al., 2013)
Consequently, advanced technology increases the importance of basic operational precision rather than replacing it.
Repeated centrifugation should therefore be understood partly as a strategy for preparing specimens suitable for increasingly sophisticated biomedical systems. The objective is not perfection in an abstract sense but reduction of avoidable uncertainty within highly sensitive analytical environments.
Within clinical trial laboratories, uncertainty carries substantial scientific consequences.
Clinical research depends fundamentally upon comparative interpretation. Investigators compare treatment groups, evaluate therapeutic responses, monitor biomarker trajectories, assess disease progression, and identify statistically meaningful differences between biological conditions. If variability introduced during specimen handling becomes sufficiently large, distinguishing genuine therapeutic effects from procedural artefacts becomes increasingly difficult.
This issue is particularly significant in translational immunology where therapeutic effects may initially appear subtle at the biomarker level.
A biologic therapy targeting inflammatory pathways in AERD may produce moderate reductions in specific cytokines or eosinophilic activity before larger clinical improvements become visible. Biomarker precision therefore becomes essential for identifying early therapeutic signals. Procedural noise introduced during plasma processing may obscure these signals entirely.
Repeated spinning attempts partly to improve signal-to-noise ratio by reducing residual biological contaminants capable of generating artificial variability.
Importantly, signal preservation does not imply eliminating all biological variability. Genuine physiological complexity remains essential scientific information. The goal is instead to reduce non-physiological variability introduced during handling so that measured changes more accurately reflect actual patient biology rather than operational inconsistency.
This distinction is central to understanding the philosophy underlying laboratory optimisation.
The purpose of repeated centrifugation is not to manufacture artificial uniformity. It is to protect authentic biological differences from being masked by avoidable procedural disturbances.
Within this context, plasma purity becomes deeply connected to interpretational reliability.
Cleaner plasma frequently produces more stable downstream analytical behaviour. Assays may demonstrate improved reproducibility. Biomarker distributions may become less erratic. Freeze-thaw stability may improve. Longitudinal comparisons may become more reliable. Inter-laboratory consistency may increase.
These improvements collectively contribute to stronger dataset integrity.
Dataset integrity refers not merely to the absence of missing values or statistical anomalies but to the broader trustworthiness of biological representation within the data itself. A high-integrity dataset reflects physiological reality as accurately as possible given existing technological and operational limitations.
The laboratory therefore participates directly in constructing interpretational confidence.
This relationship between specimen processing and scientific interpretation becomes particularly important when considering the broader biomedical research ecosystem.
Clinical trial data influences multiple downstream systems simultaneously. Pharmaceutical companies evaluate therapeutic efficacy using biomarker evidence. Regulatory agencies review laboratory findings during approval processes. Physicians interpret translational research when considering treatment strategies. Academic researchers build future hypotheses using published datasets. Artificial intelligence systems train predictive models using existing biomedical data.
Consequently, laboratory processing decisions may exert influence extending far beyond the immediate analytical environment.
The second or third spin performed quietly within a laboratory may ultimately contribute indirectly to therapeutic approval decisions, clinical guidelines, biomarker discovery, or future scientific paradigms.
This broader perspective challenges the common assumption that laboratory preparation exists merely as a technical support function beneath “real” scientific work. In reality, operational handling forms part of the epistemological foundation of biomedical science itself. It shapes how knowledge becomes generated, stabilised, and interpreted.
The issue becomes even more significant when considering reproducibility within scientific research.
Reproducibility has emerged as a major concern across multiple scientific disciplines, including biomedical research. Studies sometimes fail to reproduce expected findings despite using apparently similar analytical methods. While many factors contribute to reproducibility challenges, pre-analytical variability represents one of the most difficult sources of inconsistency to standardise fully across institutions. (Plebani, 2006)
Different laboratories may use varying centrifugation speeds, processing timelines, plasma transfer techniques, storage conditions, freeze-thaw protocols, or handling workflows even when studying similar biomarkers. Consequently, biological measurements may differ partly because specimen preparation itself differs.
Repeated spinning protocols therefore contribute not only to local sample quality but also potentially to broader inter-study reliability.
Standardisation of pre-analytical procedures becomes increasingly important as collaborative international research expands. Multi-site clinical trials frequently involve specimens collected across numerous hospitals, research centres, and countries. Ensuring consistent biological handling across geographically distributed systems becomes extraordinarily complex.
Within such environments, clearly defined plasma refinement strategies may help reduce variability between collection sites.
Another important aspect of data enhancement involves long-term biospecimen value.
Many clinical trial specimens are preserved within biobanks for future research applications extending beyond the original study objectives. Plasma collected today may later support investigations using technologies not yet available during initial processing. Future biomarker discovery often depends heavily upon historical specimen collections maintained under high-quality pre-analytical conditions. (Vaught et al., 2009; Moore et al., 2011)
Repeated centrifugation may therefore increase future scientific utility by producing specimens capable of supporting more sensitive downstream analyses over time.
This transforms the laboratory into an institution preserving future scientific possibility rather than merely processing present samples.
Within AERD research specifically, this carries significant importance because the disease remains biologically complex and incompletely understood. Emerging research continues identifying new inflammatory pathways, cellular interactions, and molecular mechanisms associated with disease progression. Archived plasma specimens processed under refined protocols may later contribute to discoveries impossible to anticipate at the time of collection.
The laboratory thus participates in both immediate clinical research and long-term scientific infrastructure simultaneously.
Yet despite this importance, much of laboratory optimisation remains comparatively invisible within published scientific literature.
Research papers frequently dedicate extensive discussion to analytical technologies, statistical methodologies, and biological findings while providing relatively limited detail regarding nuanced pre-analytical handling decisions. The labour intensity underlying specimen refinement often disappears from the visible scientific narrative despite substantially influencing data quality.
This invisibility partly reflects broader cultural tendencies within science to prioritise final analytical outputs over operational processes producing those outputs.
However, as precision medicine advances, the hidden importance of specimen integrity is becoming increasingly difficult to ignore.
Artificial intelligence-driven diagnostics, personalised inflammatory profiling, high-resolution proteomics, and biomarker-guided therapeutics all require biological inputs of exceptional consistency. The future of precision medicine will therefore depend partly upon recognising laboratory processing as a strategic scientific discipline rather than merely a technical preliminary stage.
Within this broader scientific transformation, repeated centrifugation and large component adjustment represent more than operational refinements alone.
They embody a deeper recognition that scientific truth is vulnerable during transition from living biology to measurable data. Every stage of handling introduces opportunities either to preserve or distort that truth. The laboratory exists precisely to minimise distortion.
The second spin therefore becomes symbolic of something larger within clinical research philosophy. It reflects the understanding that reliable biomedical knowledge emerges not only through analytical sophistication but through cumulative operational care applied long before the first statistical analysis begins.
Before medicine becomes data, it first passes through the hands of the laboratory.
CHAPTER 9
AERD, INFLAMMATORY NETWORKS, AND THE CHALLENGE OF MEASURING BIOLOGICAL COMPLEXITY
One of the greatest difficulties within modern immunology is that inflammation rarely behaves in simple or isolated ways. Inflammatory diseases are not linear systems governed by singular biomarkers acting independently from one another. Instead, they emerge through highly interconnected biological networks involving cellular communication, chemical signalling, tissue interactions, metabolic pathways, environmental triggers, genetic predisposition, and dynamic immunological feedback mechanisms operating simultaneously across multiple physiological layers.
Aspirin-Exacerbated Respiratory Disease (AERD) represents one of the clearest examples of this complexity.
At the clinical level, AERD is commonly characterised by a triad consisting of asthma, chronic rhinosinusitis with nasal polyps, and hypersensitivity reactions to aspirin or other cyclooxygenase-1 (COX-1) inhibiting nonsteroidal anti-inflammatory drugs (NSAIDs). Yet beneath these clinical manifestations exists a far more intricate immunological architecture involving chronic eosinophilic inflammation, dysregulated arachidonic acid metabolism, mast cell activation, platelet involvement, leukotriene overproduction, epithelial dysfunction, and persistent inflammatory amplification. (Laidlaw & Boyce, 2016; Stevens et al., 2016)
This biological complexity makes AERD both scientifically fascinating and operationally difficult to study.
Unlike diseases associated with singular dominant biomarkers, AERD involves multiple overlapping inflammatory pathways interacting dynamically over time. Cytokines influence leukocyte recruitment. Eosinophils interact with epithelial tissues. Platelets contribute to inflammatory signalling. Mast cells release mediators capable of amplifying respiratory responses. Lipid-derived inflammatory molecules such as leukotrienes alter airway behaviour dramatically. Consequently, no single laboratory measurement fully captures the totality of disease activity.
The challenge for clinical research therefore becomes one of biological representation.
How can laboratories and researchers accurately measure diseases whose underlying inflammatory behaviour continuously changes across time, tissue environments, and physiological conditions?
Blood analysis offers one important pathway toward answering this question because blood functions as a circulating informational medium connecting multiple organ systems simultaneously. Inflammatory signals generated within respiratory tissues often leave measurable traces within circulation. Cytokines, chemokines, eosinophilic proteins, platelet activation markers, prostaglandin metabolites, leukotrienes, and immunoglobulins collectively contribute fragments of information reflecting broader inflammatory processes occurring throughout the body.
However, blood also introduces interpretational limitations.
Circulating biomarkers represent indirect reflections of highly localised tissue processes. The inflammatory environment within nasal polyps, bronchial tissues, or respiratory epithelium may differ substantially from biomarker concentrations measured within plasma. Furthermore, many inflammatory signals fluctuate rapidly depending upon timing, medication exposure, disease severity, allergen interaction, respiratory stress, infection, or therapeutic intervention.
The laboratory therefore attempts to capture moving biological targets within continuously changing physiological systems.
This is precisely why pre-analytical precision becomes so important in AERD research.
When disease biology itself is already highly variable, laboratories must minimise avoidable procedural variability as much as possible. Otherwise, distinguishing genuine inflammatory behaviour from operational noise becomes increasingly difficult. Repeated centrifugation and large component adjustment emerge partly from this scientific necessity: the need to preserve biological complexity without artificially distorting it further during specimen handling.
To understand why this matters, it is necessary to examine the inflammatory mechanisms underlying AERD more closely.
A central feature of AERD involves dysregulation within arachidonic acid metabolism.
Under normal physiological conditions, arachidonic acid functions as a precursor molecule contributing to the production of multiple inflammatory mediators through competing enzymatic pathways. Cyclooxygenase (COX) pathways produce prostaglandins, while lipoxygenase pathways generate leukotrienes. In healthy systems, these pathways maintain relative balance and contribute to controlled inflammatory regulation. (Bochenek et al., 1996; Cahill & Boyce, 2014)
In AERD, however, this balance becomes disrupted.
When patients with AERD are exposed to aspirin or other COX-1 inhibiting NSAIDs, protective prostaglandin synthesis decreases while leukotriene production becomes amplified disproportionately. Leukotrienes are potent inflammatory mediators capable of inducing bronchoconstriction, mucus production, vascular permeability, eosinophilic recruitment, and airway inflammation.
The result is an exaggerated inflammatory cascade affecting respiratory function dramatically.
Importantly, this leukotriene-driven inflammatory amplification does not occur in isolation. Multiple cellular systems participate simultaneously. Eosinophils infiltrate respiratory tissues. Mast cells release histamine and inflammatory mediators. Platelets interact with leukocytes. Cytokines coordinate ongoing immune recruitment and signalling.
The inflammatory network therefore becomes self-reinforcing.
This complexity creates significant challenges for laboratory measurement because biomarkers associated with these pathways often demonstrate dynamic interdependence rather than stable isolated behaviour. A shift in one inflammatory mediator may trigger downstream changes across numerous related pathways. Timing therefore becomes critically important when collecting and processing specimens.
For example, cytokine concentrations may rise transiently during acute inflammatory activation and decline rapidly thereafter. Certain leukotrienes degrade relatively quickly under improper handling conditions. Platelet activation may continue after collection if plasma processing is delayed or incomplete. Consequently, the biological state of the sample at the time of laboratory analysis may differ substantially from its original physiological condition if pre-analytical handling is not carefully controlled.
Repeated spinning attempts partly to protect against these distortions by reducing residual cellular contamination capable of altering inflammatory composition during storage and handling.
Platelets represent an especially important consideration in this context.
Historically, platelets were viewed primarily through the lens of coagulation biology. However, modern immunology increasingly recognises platelets as active inflammatory participants involved in immune signalling, leukocyte recruitment, vascular inflammation, and disease modulation. In AERD specifically, platelet-leukocyte aggregates have attracted growing research attention due to their contribution to leukotriene pathway dysregulation. (Semple et al., 2011; Gros et al., 2014)
Residual platelets suspended within incompletely processed plasma may therefore continue releasing inflammatory mediators after collection, potentially altering biomarker profiles artificially.
This introduces an important conceptual issue within laboratory medicine.
Biomarker measurements do not simply reflect disease biology. They reflect disease biology as preserved—or altered—through laboratory processing systems.
The distinction may appear subtle, but scientifically it is profound.
A cytokine concentration measured during downstream analysis is not merely a passive observation of patient physiology untouched by handling. It is the final outcome of multiple interacting processes including collection timing, transport stability, centrifugation efficiency, plasma purity, storage integrity, freeze-thaw exposure, and analytical sensitivity.
The laboratory therefore participates actively in constructing the conditions under which biological complexity becomes measurable.
This becomes especially relevant when studying diseases such as AERD where inflammatory behaviour is inherently nonlinear.
Nonlinear biological systems do not behave predictably according to simple cause-and-effect relationships. Small changes may produce disproportionately large downstream effects. Feedback loops amplify inflammatory responses. Cellular interactions evolve dynamically over time. Consequently, biomarker interpretation requires careful awareness of both biological and procedural complexity simultaneously.
Clinical trial laboratories therefore occupy a difficult scientific position.
They must preserve enough biological complexity to maintain meaningful disease representation while simultaneously reducing procedural noise capable of obscuring interpretational clarity. Over-processing risks damaging fragile biomarkers. Under-processing risks residual contamination. Standardisation promotes consistency but may not fully account for individual specimen variability.
The laboratory continuously negotiates between these competing pressures.
Within AERD research, this negotiation becomes particularly challenging because patients themselves often exhibit highly heterogeneous disease behaviour.
Some individuals experience severe respiratory reactivity with extensive eosinophilic inflammation. Others demonstrate differing inflammatory profiles despite similar clinical diagnoses. Medication exposure varies. Steroid treatment influences biomarker concentrations. Chronic sinus disease contributes additional inflammatory complexity. Coexisting allergic conditions may further modify immune behaviour.
Consequently, laboratory specimens arriving from different patients may behave very differently during processing.
Some plasma samples appear exceptionally clear after initial centrifugation. Others retain persistent turbidity or particulate suspension despite standard protocols. Lipid concentrations, inflammatory protein burden, clotting tendencies, and medication effects all influence specimen characteristics.
Experienced laboratory personnel often begin recognising these patterns intuitively over time.
This experiential familiarity forms an important but rarely acknowledged dimension of translational immunology research. Scientific understanding emerges not only from formal experimental design but also from repeated operational engagement with biological variability itself.
Repeated spinning protocols reflect this practical recognition that certain specimens require additional refinement to preserve analytical integrity adequately.
Importantly, the objective of repeated centrifugation is not to remove meaningful biology but to reduce unwanted interference obscuring meaningful biology.
This distinction becomes especially important when discussing inflammatory diseases because some critics may worry that excessive processing could potentially alter native biomarker environments artificially. Such concerns are scientifically valid. Overly aggressive handling may indeed damage fragile analytes or introduce mechanical stress.
However, carefully calibrated repeated spinning seeks not to manipulate inflammatory signals but to stabilise them against ongoing ex vivo biological activity occurring after collection.
The second or third spin therefore functions partly as a protective intervention preserving the closest possible approximation of the original physiological state.
This protective philosophy aligns closely with broader goals within precision medicine.
Modern medicine increasingly seeks to classify patients according to molecular and immunological characteristics rather than broad symptom categories alone. Biomarker-driven therapeutics depend heavily upon accurate inflammatory profiling. Biological therapies targeting specific cytokines, eosinophilic pathways, or inflammatory mediators require precise laboratory assessment to evaluate treatment response properly.
In diseases such as AERD, where inflammatory networks are especially intricate, biomarker reliability becomes central to therapeutic development itself.
Consequently, the laboratory occupies an increasingly strategic role within translational medicine ecosystems.
It is no longer sufficient for laboratories merely to process samples according to generic clinical standards. Research-grade immunological analysis increasingly demands advanced specimen refinement strategies capable of supporting ultra-sensitive biomarker evaluation.
Repeated centrifugation and large component adjustment represent part of this broader evolution toward research-oriented laboratory optimisation.
The implications extend beyond immediate clinical trials.
As artificial intelligence, machine learning, and computational biomarker modelling become more integrated into biomedical research, the quality of training data becomes critically important. AI systems learn patterns from existing datasets. If those datasets contain hidden pre-analytical variability introduced during specimen handling, computational interpretation may inherit procedural distortions unknowingly.
The future of computational medicine therefore remains deeply dependent upon biological sample integrity.
No algorithm, regardless of sophistication, can fully recover biological information lost during improper specimen processing.
This reality reinforces a central argument underlying modern laboratory optimisation: that operational precision is not secondary to scientific discovery but foundational to it.
Within AERD research, repeated spinning ultimately reflects an attempt to protect biological truth within systems vulnerable to instability at every stage of handling.
The laboratory cannot eliminate the complexity of inflammatory disease. Nor should it attempt to do so. Complexity itself contains valuable scientific information. However, the laboratory can attempt to prevent additional artificial complexity from obscuring meaningful biological patterns.
This is the deeper purpose of large component adjustment.
It is not simply about cleaner plasma or improved centrifugation technique. It is about preserving the integrity of inflammatory information long enough for medicine to learn from it accurately.
In diseases governed by hidden inflammatory networks, even the quiet rotation of a centrifuge may shape how biological complexity becomes understood.
CHAPTER 10
THE LABORATORY, TRANSLATIONAL MEDICINE, AND THE FUTURE OF PRECISION IMMUNOLOGY
The history of medicine is often narrated through visible breakthroughs. Scientific revolutions are associated with vaccines, antibiotics, organ transplantation, imaging technologies, monoclonal antibodies, genomic sequencing, and advanced therapeutics capable of transforming once-fatal diseases into manageable clinical conditions. Yet behind nearly every major biomedical advancement exists another quieter history—one shaped not by dramatic interventions alone but by gradual improvements in the ability to measure, preserve, interpret, and stabilise biological information.
Modern medicine advances when biology becomes measurable with increasing reliability.
This process of measurement depends fundamentally upon laboratories.
Clinical laboratories have historically occupied an unusual position within healthcare systems. They are simultaneously central and invisible. Physicians depend upon laboratory results continuously. Pharmaceutical companies build therapeutic development pipelines around biomarker evidence. Regulatory agencies evaluate clinical trial outcomes using laboratory-generated data. Researchers construct scientific theories from measurable biological patterns. Yet despite this dependence, laboratory work itself often remains hidden beneath the surface of visible medical practice.
The public sees the diagnosis but not the centrifuge.
They see the treatment outcome but not the plasma preparation.
They see the biomarker graph but not the pre-analytical handling that made the graph possible.
As biomedical science moves increasingly toward precision medicine and immunologically targeted therapeutics, this invisibility is becoming progressively harder to sustain.
Precision medicine depends upon the assumption that diseases can be understood and treated according to highly specific molecular, genetic, inflammatory, or immunological characteristics unique to individual patients. Instead of grouping all patients with similar symptoms into broad categories, precision medicine seeks to identify biologically distinct subtypes, inflammatory signatures, and molecular pathways driving disease behaviour.
This transformation fundamentally increases the importance of laboratory science.
Traditional medicine frequently relied upon relatively broad clinical observations. Precision medicine, by contrast, depends upon extraordinarily sensitive biological measurements capable of detecting subtle molecular differences between individuals. Cytokine profiles, proteomic patterns, genomic variations, metabolomic signatures, eosinophilic activity, immune phenotypes, and inflammatory pathway interactions all become increasingly relevant.
However, the more sensitive biomedical analysis becomes, the more vulnerable it becomes to pre-analytical inconsistency.
This creates one of the defining paradoxes of modern translational medicine.
Advanced analytical technologies are often celebrated as though technological sophistication alone guarantees scientific progress. Yet increasingly sensitive systems also magnify the consequences of improper specimen handling. Minor residual contamination previously undetectable under older methodologies may now influence downstream interpretation significantly. Small inconsistencies in centrifugation, storage, freeze-thaw exposure, or plasma refinement may distort highly sensitive biomarker profiles.
Consequently, the future of precision medicine depends not only upon analytical innovation but also upon operational refinement. (Collins & Varmus, 2015; Fauci & Collins, 2016)
Repeated centrifugation and large component adjustment should therefore be understood within this larger biomedical transformation. They represent part of a broader movement toward preserving biological integrity in environments where analytical sensitivity continues increasing rapidly.
Within allergy and immunology research involving diseases such as Aspirin-Exacerbated Respiratory Disease (AERD), this issue becomes especially important because inflammatory biology is inherently dynamic, multidimensional, and context-dependent.
AERD is not a disease easily reduced to singular biomarkers or simple inflammatory pathways. Rather, it reflects interacting networks involving leukotriene dysregulation, eosinophilic inflammation, mast cell activation, platelet-leukocyte interactions, cytokine signalling, respiratory tissue remodelling, and chronic immune amplification. Different patients may exhibit varying inflammatory dominance patterns despite sharing similar clinical diagnoses.
The challenge for precision immunology is therefore not merely detecting inflammation but characterising its specific biological architecture accurately.
This requires highly reliable biospecimens.
Repeated spinning contributes to this reliability by improving plasma purity and reducing residual biological interference capable of obscuring subtle inflammatory patterns. Cleaner plasma enhances the ability of downstream analytical systems to detect authentic biological signals rather than procedural artefacts. In this sense, large component adjustment functions partly as a preparatory technology for precision medicine itself.
The relationship between specimen quality and translational medicine becomes even clearer when examining the development of biologic therapies.
Modern immunology increasingly relies upon targeted biologics designed to inhibit highly specific inflammatory mediators. Therapies targeting interleukins, eosinophilic pathways, IgE signalling, leukotriene mechanisms, or inflammatory receptors require detailed biomarker assessment throughout clinical development. Investigators must determine which inflammatory pathways dominate disease activity, how biomarker profiles shift following therapy, and which patients are most likely to respond.
Laboratory measurements therefore influence not only scientific understanding but also therapeutic strategy.
A biomarker trend observed during a clinical trial may shape decisions regarding drug efficacy, dosing protocols, patient selection criteria, or future regulatory approval pathways. Consequently, the integrity of laboratory processing becomes deeply connected to pharmaceutical development itself.
Within this framework, the clinical trial laboratory should no longer be viewed merely as a technical support environment subordinate to “real” clinical science. It is an active translational interface where biological complexity becomes converted into actionable medical evidence.
This translational role continues expanding as immunological medicine evolves.
Historically, many diseases were classified primarily according to anatomical symptoms or broad physiological dysfunction. Today, however, increasing emphasis is placed upon molecular phenotyping and inflammatory endotyping. Asthma itself is now understood as biologically heterogeneous rather than singular. Similar symptomatic presentations may arise through entirely different inflammatory mechanisms across different individuals.
AERD illustrates this shift particularly well.
Although clinically associated with respiratory symptoms and aspirin sensitivity, underlying inflammatory behaviour varies considerably between patients. Some individuals demonstrate profound eosinophilic dominance. Others exhibit stronger mast cell activity or differing cytokine environments. Therapeutic response similarly varies depending upon these underlying biological characteristics.
The laboratory therefore becomes essential for identifying hidden inflammatory diversity beneath visible clinical similarity.
Repeated centrifugation supports this objective indirectly by improving the reliability of biomarker-driven interpretation.
Importantly, this issue extends beyond current analytical technologies alone.
Future biomedical systems will likely become even more dependent upon high-integrity biospecimens. Artificial intelligence-assisted diagnostics, machine learning biomarker prediction models, digital pathology integration, single-cell analysis, spatial transcriptomics, ultra-sensitive proteomics, and multi-omic data integration all require exceptionally stable biological inputs. (Collins & Varmus, 2015)
The future of computational medicine therefore remains inseparable from the future of laboratory handling.
Artificial intelligence systems, regardless of sophistication, cannot fully compensate for compromised biospecimen quality. Algorithms learn patterns from available data. If pre-analytical variability introduces hidden distortions into biomarker datasets, AI systems may unknowingly incorporate procedural artefacts into predictive models.
Consequently, operational precision within the laboratory may become increasingly important in the era of biomedical artificial intelligence rather than less.
This represents a major conceptual shift within modern science.
Traditionally, technological progress is often imagined as replacing manual operational importance. However, in laboratory medicine, increasing technological sensitivity frequently increases the value of careful specimen handling because more delicate analytical systems require higher-quality biological inputs.
The centrifuge therefore remains deeply relevant even within futuristic biomedical landscapes.
Repeated spinning, plasma refinement, and large component adjustment may appear comparatively simple compared to genomic sequencing or machine learning platforms. Yet these foundational procedures help determine whether downstream technologies receive biologically reliable material in the first place.
The future of precision immunology therefore depends partly upon recognising the strategic importance of pre-analytical science.
Another important dimension of translational medicine involves longitudinal biospecimen preservation.
Many clinical trial specimens are stored for years within biobanks supporting future investigations beyond the original research objectives. Plasma collected today may eventually undergo analyses using technologies not yet invented at the time of collection. Future discoveries regarding inflammatory pathways, biomarker interactions, or disease mechanisms may depend upon archived specimens processed decades earlier.
This gives laboratory preparation enduring scientific consequences.
A specimen inadequately processed today may lose future analytical value permanently. Conversely, high-quality plasma refinement may preserve biological integrity sufficient for future translational discovery. (Vaught et al., 2009; Moore et al., 2011)
Repeated spinning therefore contributes not only to immediate assay performance but also to long-term biomedical infrastructure.
Within AERD research, this carries particular significance because the disease continues evolving scientifically. New inflammatory mechanisms are still being identified. The role of platelets, epithelial dysfunction, lipid mediators, cytokine networks, and immune signalling pathways remains under active investigation. Preserved plasma samples from contemporary clinical trials may later contribute to scientific insights impossible to anticipate fully today.
The laboratory thus becomes partly an archive of future medical possibility.
Yet despite this importance, operational laboratory science often remains underrepresented within broader academic narratives.
Research publications frequently focus heavily on biological findings while devoting comparatively little attention to the procedural environments producing those findings. Methods sections may briefly mention centrifugation protocols without discussing the practical realities of plasma refinement, handling complexity, workflow coordination, or pre-analytical vulnerability.
This invisibility partly reflects longstanding cultural hierarchies within science where analytical interpretation receives greater recognition than operational preparation.
However, the future trajectory of translational medicine may gradually challenge this hierarchy.
As precision medicine advances, specimen integrity increasingly becomes impossible to separate from interpretational validity. The distinction between laboratory operations and scientific discovery becomes less clear because operational decisions actively shape the biological information available for analysis.
Repeated spinning therefore symbolises something larger than centrifugation alone.
It represents a broader scientific philosophy recognising that biomedical truth is fragile during transition from living physiology to measurable data. Every stage of handling introduces opportunities either to preserve or distort that truth. The laboratory exists to reduce distortion as much as possible while preserving meaningful biological complexity.
This philosophy becomes especially important in immunology where inflammation itself is dynamic, context-dependent, and continuously evolving.
Within diseases such as AERD, biomarkers are not static chemical entities existing independently from biological systems. They emerge through living inflammatory networks interacting across time. The laboratory must therefore preserve not only isolated molecules but relationships between inflammatory processes themselves.
Repeated centrifugation contributes to this preservation by reducing residual biological activity capable of altering inflammatory composition after collection.
The second spin thus becomes more than a procedural repetition. It becomes part of a broader effort to stabilise biological reality long enough for medicine to study it accurately.
Ultimately, the future of precision immunology will depend not only upon discovering new biomarkers or developing more advanced analytical technologies. It will also depend upon improving the integrity of the pathways through which biology becomes measurable in the first place.
Long before medicine becomes personalised, targeted, computational, or predictive, it must first remain biologically trustworthy inside the laboratory tube.
The future of translational medicine therefore begins quietly, in the controlled rotation of the centrifuge.
CHAPTER 11
THE HUMAN DIMENSION OF LABORATORY SCIENCE
Scientific research is frequently portrayed as an intellectual pursuit dominated by theories, data, experiments, technologies, and discoveries. Biomedical science, in particular, is often represented through images of advanced instrumentation, molecular pathways, computational analysis, and pharmaceutical innovation. Yet beneath these visible layers exists another reality rarely discussed with equal seriousness: the human labour sustaining the precision of scientific systems themselves.
Clinical laboratories do not operate autonomously.
Centrifuges do not prepare specimens independently.
Biomarkers do not preserve themselves.
Data does not emerge spontaneously from blood.
Behind every stable plasma aliquot, every cytokine dataset, every inflammatory profile, and every clinical trial result exists an environment shaped by human concentration, repetition, discipline, technical dexterity, emotional endurance, and operational consistency.
This human dimension of laboratory science remains one of the most invisible yet foundational aspects of modern medicine.
Within clinical trial laboratories studying diseases such as Aspirin-Exacerbated Respiratory Disease (AERD), this invisibility becomes especially striking because the work itself is often highly repetitive, procedural, and physically demanding despite carrying substantial scientific significance. Personnel spend long hours processing specimens, operating centrifuges, aliquoting plasma, organising freezers, documenting handling timelines, monitoring temperatures, balancing workflow priorities, and maintaining procedural consistency across hundreds of samples.
To outsiders, these activities may appear routine. However, routine within laboratory environments is not simplicity. It is disciplined repetition under conditions where small inconsistencies may carry disproportionate scientific consequences.
This distinction is deeply important.
The precision demanded within laboratory medicine is psychologically different from many other forms of professional work because errors often remain invisible initially. A poorly processed specimen may still appear acceptable. A slightly disturbed buffy coat may not immediately reveal downstream contamination. A delayed centrifugation window may not produce obvious visible change. Yet subtle procedural deviations may later influence cytokine measurements, biomarker stability, inflammatory profiles, or statistical interpretation in ways difficult to trace retrospectively.
Laboratory personnel therefore work within systems where the consequences of small actions may only emerge much later through analytical interpretation.
This creates a unique psychological environment characterised by sustained vigilance.
Unlike professions driven primarily by dramatic decision-making moments, laboratory science depends heavily upon maintaining concentration across repetitive procedural sequences. The same actions must be performed consistently again and again despite fatigue, interruptions, workflow congestion, and operational pressure.
Pipetting plasma from above the buffy coat may appear simple when described within protocols. In practice, maintaining perfect consistency across hundreds of specimens requires substantial attentional discipline. Slight variations in hand angle, pipette depth, aspiration speed, or tube positioning may influence residual contamination subtly.
Repeated spinning protocols intensify this requirement because additional handling stages create more opportunities for disturbance.
The second spin itself is relatively straightforward mechanically. However, everything surrounding the second spin requires coordination: plasma transfer timing, centrifuge availability, sample tracking, aliquot preparation, freezer management, documentation accuracy, and workflow synchronisation. Scientific reliability therefore emerges through cumulative procedural consistency rather than isolated technical moments alone.
This cumulative nature of precision is central to understanding laboratory work.
No single perfectly executed action guarantees specimen integrity. Rather, integrity depends upon maintaining acceptable consistency across long chains of operational behaviour. A high-quality plasma sample reflects not one action but dozens of correctly performed actions occurring sequentially without major disruption.
The laboratory thus functions partly as a system of behavioural discipline.
Personnel develop highly structured routines partly because routine reduces variability. Tube placement becomes systematic. Pipette organisation becomes intentional. Documentation sequences become habitual. Timing awareness becomes almost instinctive. Repetition gradually transforms procedural consistency into embodied operational memory.
This process resembles forms of disciplined craftsmanship more than many people realise.
Laboratory expertise is not purely intellectual knowledge stored abstractly in the mind. It also becomes physical knowledge expressed through movement, posture, timing, hand stability, spatial organisation, and sensory familiarity with specimen behaviour.
Experienced laboratory professionals often recognise abnormalities almost intuitively. Slight plasma haze, delayed separation, fibrin traces, haemolysis colouration, lipaemic appearance, or unusual specimen viscosity may become immediately noticeable even before formal analysis begins.
This observational sensitivity develops through prolonged immersion in specimen processing environments.
Yet despite requiring substantial expertise, laboratory labour frequently remains socially invisible within healthcare systems.
Patients rarely meet the personnel processing their blood samples. Clinical trial publications seldom acknowledge the operational intensity underlying specimen preparation. Scientific recognition tends to concentrate around principal investigators, analytical findings, or therapeutic outcomes rather than the individuals sustaining pre-analytical integrity behind the scenes.
This invisibility contributes partly to a broader misunderstanding regarding where scientific value is produced.
Biomedical research is often imagined as occurring primarily during data analysis or theoretical interpretation. However, data itself only becomes scientifically meaningful if the biological material generating that data remains trustworthy. Laboratory personnel therefore participate directly in knowledge production even when their labour remains absent from visible scientific narratives.
The invisibility of laboratory work also shapes the emotional experience of laboratory professionals themselves.
Unlike physicians or nurses who interact directly with patients and witness immediate clinical outcomes, laboratory personnel frequently work at a distance from visible therapeutic impact. Their contribution is indirect yet essential. They may never meet the patients whose inflammatory biomarkers they process daily. They may never observe the eventual therapeutic outcomes influenced by the datasets they help preserve.
Yet the responsibility remains profound.
Every specimen represents a patient participating in scientific research, often under conditions of chronic illness, uncertainty, or therapeutic hope. Within AERD research, many individuals entering clinical trials have experienced years of respiratory distress, recurrent sinus surgery, medication side effects, chronic inflammation, and disrupted quality of life.
The laboratory therefore handles not merely biological material but evidence of lived disease experience.
This reality creates a subtle ethical dimension within specimen handling.
Operational precision becomes more than procedural compliance. It becomes a form of responsibility toward the individuals whose biology is being translated into scientific evidence. Maintaining specimen integrity is not only scientifically important but ethically important because patients participate in clinical research with expectation that their contributions will be handled carefully and meaningfully.
Repeated centrifugation may therefore be understood partly as an ethical practice of care within translational medicine.
The second or third spin reflects additional effort invested toward preserving analytical reliability. It represents recognition that small operational refinements may improve the scientific value of patient-derived specimens.
This perspective humanises laboratory optimisation in an important way.
Discussions of centrifugation often focus heavily on technical parameters: relative centrifugal force, platelet reduction, plasma purity, biomarker stability, or signal-to-noise improvement. These scientific considerations are essential. However, behind them exists another quieter reality: laboratory personnel repeatedly performing careful procedural work because they understand that biological information is fragile.
The fragility of biological information shapes much of laboratory psychology.
Blood appears physically stable when viewed casually. Tubes sit quietly within racks. Plasma remains visually still after centrifugation. Yet laboratory professionals understand that beneath this apparent stability, biological degradation continues continuously unless carefully controlled.
Proteins degrade. Cells activate. Cytokines fluctuate. Freeze-thaw instability alters composition. Time itself becomes an active force acting against specimen integrity.
The laboratory therefore functions partly as an environment resisting biological decay long enough for scientific interpretation to occur.
This creates a peculiar relationship between time and labour within clinical laboratories.
Personnel constantly work against temporal deterioration. Specimens must move rapidly through processing stages before instability emerges. Delays accumulate risk. Workflow interruptions threaten timelines. Equipment malfunction becomes urgent not merely operationally but biologically.
The pace of laboratory work is therefore dictated partly by the instability of living systems once removed from physiological regulation.
Repeated spinning protocols complicate this further because additional refinement requires additional time while simultaneously attempting to improve long-term stability. Laboratories must therefore balance immediate processing speed against downstream analytical quality.
This balance reflects a larger tension within biomedical research between efficiency and precision.
Modern healthcare systems frequently prioritise throughput, productivity, automation, and scalability. Laboratories process increasingly large specimen volumes under substantial operational pressure. However, highly sensitive immunological research often demands slower and more careful handling than industrial efficiency models naturally favour.
Repeated centrifugation symbolises this tension clearly.
From a purely efficiency-driven perspective, additional spins consume time and labour resources. From a scientific reliability perspective, however, they may substantially improve plasma quality and biomarker preservation.
Laboratory personnel therefore continuously navigate competing institutional pressures involving speed, consistency, workload, and analytical integrity simultaneously.
Fatigue becomes an important but rarely acknowledged factor within this environment.
Long hours of repetitive precision work require sustained concentration difficult to maintain indefinitely. Pipetting, aliquoting, centrifuge balancing, freezer organisation, documentation, and specimen handling may appear physically light compared to some forms of labour, yet cognitively and neurologically they are highly demanding because errors must remain minimised continuously.
Cognitive fatigue within laboratory settings is particularly dangerous precisely because procedures become familiar.
Repetition increases operational fluency but may also encourage automatic behaviour where actions occur with reduced conscious attention. Laboratories therefore cultivate procedural discipline intentionally to resist complacency. Checklists, verification systems, documentation protocols, and standardised workflows exist partly to protect against the cognitive vulnerabilities inherent within repetitive environments.
The psychology of precision thus becomes central to laboratory science.
Precision is not merely technical capability. It is sustained behavioural discipline under conditions where biological fragility, operational repetition, and invisible consequences coexist simultaneously.
Importantly, this human dimension will likely become even more important in the future of precision medicine.
As analytical technologies become increasingly sensitive, the quality of pre-analytical handling grows more consequential. Artificial intelligence-assisted biomarker analysis, multi-omic integration, personalised inflammatory profiling, and ultra-sensitive immunological assays all require exceptionally stable biological inputs.
The future of biomedical science therefore depends not only upon better machines but also upon preserving human operational expertise capable of maintaining specimen integrity.
Automation may reduce some manual variability, but biological systems remain complex, context-dependent, and often unpredictable. Human judgement continues playing important roles in recognising specimen abnormalities, adapting workflows, responding to unexpected conditions, and preserving procedural quality under real-world operational complexity.
The centrifuge itself illustrates this relationship between technology and human discipline.
A centrifuge can generate rotational force automatically. However, deciding how specimens should be handled before and after centrifugation, recognising whether plasma refinement is sufficient, balancing workflow timing, preserving specimen stability, and interpreting operational context all still depend heavily upon human expertise.
Large component adjustment therefore reflects not only a technical methodology but also a philosophy of attentiveness within laboratory science.
The second spin symbolises patience against haste.
It symbolises refinement against approximation.
It symbolises the recognition that biological information deserves careful handling because scientific interpretation depends upon it.
Within the quiet operational spaces of the clinical trial laboratory, precision is sustained not through dramatic scientific moments but through disciplined repetition performed day after day, specimen after specimen, often without visibility or recognition.
Yet modern medicine depends upon this invisible labour more than it frequently acknowledges.
Before biomarkers become discoveries, before datasets become publications, and before therapies become approved treatments, biological truth must first survive the hands of the laboratory worker.
CHAPTER 12
LARGE COMPONENT ADJUSTMENT AS A SCIENTIFIC FRAMEWORK
Within most conventional laboratory protocols, centrifugation is described operationally rather than conceptually. Procedures specify rotational speeds, spin durations, temperature settings, and plasma transfer instructions, but rarely frame centrifugation itself as a broader scientific philosophy influencing how biomedical information is preserved and interpreted. The process is often treated as a necessary technical routine preceding “real” analytical work rather than an active contributor to scientific validity.
However, repeated centrifugation and large component adjustment suggest a different way of understanding laboratory processing.
They suggest that pre-analytical handling should not merely be viewed as procedural preparation but as an independent scientific framework concerned with the preservation, refinement, stabilisation, and protection of biological information before analysis occurs.
This distinction is important because the future of biomedical science increasingly depends upon pre-analytical precision.
Historically, many laboratory tests were relatively robust against minor handling inconsistencies. Basic clinical chemistry assays measuring stable analytes often tolerated modest procedural variability without dramatic interpretational consequences. However, modern immunology, translational medicine, proteomics, metabolomics, and biomarker-driven therapeutics increasingly rely upon highly sensitive biological measurements vulnerable to even subtle disturbances during specimen handling.
Consequently, the conceptual importance of large component adjustment extends beyond repeated spinning alone.
It represents a broader recognition that biological specimens are not passive objects moving through laboratories unchanged. They are dynamic molecular environments continuously responding to handling conditions, temperature exposure, mechanical stress, timing delays, residual cellular activity, and storage instability. The laboratory therefore becomes a site where biological reality is either preserved carefully or gradually altered through procedural neglect.
Large component adjustment emerges from this awareness.
At its most practical level, large component adjustment refers to the progressive refinement of plasma through repeated centrifugation cycles designed to reduce residual platelets, leukocytes, fibrin traces, cellular debris, and other suspended particulates capable of interfering with downstream analysis. Yet conceptually, it reflects something much larger: the attempt to minimise avoidable biological distortion during the transition from living physiology to measurable scientific data.
This transition is one of the most vulnerable stages within biomedical research.
Blood inside the body exists under tightly regulated physiological conditions. Temperature, pH balance, oxygenation, hormonal signalling, vascular flow, and cellular interactions continuously maintain systemic stability. Once blood is collected into laboratory tubes, however, these stabilising systems disappear almost immediately. Biological materials continue reacting despite no longer being physiologically regulated.
Cells remain alive transiently.
Platelets remain reactive.
Proteins remain vulnerable.
Inflammatory pathways continue fluctuating.
Time itself begins transforming the specimen.
The role of pre-analytical optimisation is therefore fundamentally preservational rather than merely procedural.
Repeated spinning contributes to preservation by reducing residual biological activity capable of altering plasma composition after collection. The second spin attempts to remove platelets still suspended following primary separation. The third spin may further reduce microscopic particulate contamination affecting highly sensitive assays. Each additional refinement stage represents an effort to preserve the closest possible approximation of the specimen’s original physiological state.
Importantly, this process should not be misunderstood as artificial manipulation of biology.
The objective of large component adjustment is not to create artificially “perfect” specimens detached from real physiology. Rather, it seeks to reduce unwanted ex vivo alterations occurring after blood collection so that downstream measurements more accurately reflect in vivo biological conditions at the time of venepuncture.
This distinction becomes especially significant in diseases involving chronic inflammatory instability such as Aspirin-Exacerbated Respiratory Disease (AERD).
AERD is characterised by dynamic immunological behaviour involving eosinophilic activation, leukotriene dysregulation, mast cell signalling, platelet interaction, cytokine fluctuation, and respiratory inflammation. Biomarkers associated with these pathways often exist within delicate and rapidly changing molecular environments.
If residual inflammatory cells remain within incompletely processed plasma, they may continue secreting cytokines or inflammatory mediators after collection. Measured biomarker concentrations may therefore reflect not only patient biology but also ongoing biological activity occurring inside the tube itself during handling and storage.
Large component adjustment attempts to interrupt this post-collection instability.
The significance of this process increases substantially within modern translational medicine because clinical decisions, therapeutic development, and pharmaceutical evaluation increasingly depend upon subtle biomarker interpretation.
In earlier eras of medicine, diagnosis relied heavily upon visible clinical symptoms and broad physiological patterns. Today, however, diseases are increasingly characterised through molecular signatures, inflammatory phenotypes, immune profiles, and biomarker-defined pathways. Small biological differences now carry major clinical implications.
Consequently, preserving biomarker fidelity becomes strategically important.
A slight cytokine shift may influence interpretation regarding therapeutic response. Subtle inflammatory reductions may determine whether investigational drugs proceed through development pipelines. Platelet contamination may obscure meaningful biomarker trends. Hidden pre-analytical variability may weaken reproducibility between studies.
The laboratory therefore participates directly in constructing the reliability of biomedical evidence itself.
This reality challenges traditional assumptions regarding where scientific knowledge is produced.
Knowledge is often imagined as emerging primarily during statistical analysis or theoretical interpretation. Yet before data can be analysed, it must first survive biological instability long enough to become measurable. The pre-analytical phase therefore shapes the conditions under which knowledge becomes possible.
Large component adjustment should thus be understood partly as an epistemological framework within laboratory science.
Epistemology concerns how knowledge is generated, stabilised, and validated. In biomedical research, specimen handling influences what ultimately becomes accepted as biological truth. Poorly preserved specimens may generate misleading conclusions despite highly sophisticated downstream analysis. Conversely, carefully refined plasma may improve the reliability of entire translational research systems.
The centrifuge therefore occupies a far more philosophically significant role than commonly acknowledged.
It functions not only as a mechanical separator but as an instrument mediating between unstable biology and stable scientific representation.
Repeated spinning symbolises this mediation process clearly.
The first spin performs broad separation.
The second spin refines.
The third spin stabilises further.
Each stage attempts to reduce uncertainty incrementally.
This incremental refinement parallels broader scientific methodology itself.
Science frequently advances not through singular dramatic breakthroughs alone but through gradual reduction of uncertainty across multiple operational layers. Precision emerges cumulatively. Reliability accumulates through repeated procedural care. Large component adjustment reflects this principle operationally within the laboratory.
Another important dimension of this framework involves the distinction between visible and invisible contamination.
Laboratory personnel often evaluate plasma visually following centrifugation. Clear plasma generally suggests successful separation. However, many forms of biologically significant contamination remain invisible macroscopically. Residual platelets, microparticles, inflammatory proteins, cellular fragments, and soluble mediators may persist despite visually acceptable specimens.
This invisibility is scientifically important because downstream assays may still detect the effects of these residual materials.
Repeated centrifugation partly addresses this challenge by refining plasma beyond what visual assessment alone can guarantee.
In highly sensitive immunological analysis, microscopic purity becomes increasingly relevant. Technologies such as multiplex cytokine assays, proteomic platforms, metabolomics, mass spectrometry, and high-sensitivity inflammatory profiling all amplify the consequences of subtle pre-analytical inconsistencies.
Thus, large component adjustment anticipates the needs of future analytical systems rather than belonging solely to traditional laboratory methodology.
As biomedical science advances toward ultra-sensitive molecular detection, pre-analytical optimisation will likely become increasingly central rather than peripheral.
The future laboratory may therefore place greater emphasis upon biospecimen engineering—the deliberate design of handling systems aimed at preserving biological information under increasingly demanding analytical conditions.
Large component adjustment already represents an early form of this approach.
Importantly, this framework also intersects with broader concerns regarding scientific reproducibility.
Modern biomedical research faces ongoing challenges related to reproducibility across laboratories and institutions. Findings sometimes fail replication despite apparently similar methodologies. While numerous factors contribute to reproducibility problems, pre-analytical variability remains one of the most underestimated.
Different laboratories often use different centrifugation conditions, plasma transfer methods, storage protocols, freeze-thaw practices, and handling timelines. Even small inconsistencies may influence sensitive biomarker measurements significantly.
Consequently, standardising large component adjustment methodologies may improve inter-study consistency within translational immunology research.
This is particularly relevant in multicentre clinical trials where biospecimens are collected across geographically distributed institutions. Harmonised plasma refinement protocols may help reduce hidden variability between sites and strengthen comparative reliability.
The implications extend beyond present clinical trials alone.
Biobanking increasingly preserves specimens for future analysis using technologies not yet available during initial collection. Plasma processed today may later undergo analyses unimaginable at the time of storage. Therefore, high-quality pre-analytical refinement enhances not only immediate analytical performance but also future scientific utility.
Repeated spinning may thus contribute to long-term biospecimen resilience.
This concept of resilience is important.
A resilient biospecimen maintains analytical integrity across time, storage, transport, technological evolution, and repeated investigation. The better plasma is preserved initially, the more future scientific possibilities remain accessible.
Large component adjustment therefore functions partly as an investment in future translational capacity.
Within AERD research, this is especially meaningful because the disease continues evolving scientifically. New inflammatory pathways, platelet interactions, epithelial dysfunction mechanisms, and cytokine relationships continue emerging through ongoing research. Archived plasma refined under high-quality protocols may later contribute to discoveries impossible to predict presently.
The laboratory thus participates simultaneously in present science and future scientific potential.
Yet despite these implications, pre-analytical optimisation remains comparatively under-theorised within biomedical literature.
Methods sections frequently describe centrifugation mechanically without exploring its broader conceptual significance. Laboratory refinement is often framed as technical support rather than scientific infrastructure. This reflects longstanding hierarchies within science privileging visible analytical outputs over operational processes enabling those outputs.
However, modern translational medicine increasingly destabilises this hierarchy.
As biomarkers become more sensitive and therapeutic decisions more dependent upon subtle molecular interpretation, operational refinement becomes inseparable from analytical validity itself.
The future of immunology therefore may require rethinking the laboratory not merely as a site of specimen processing but as a site of biological preservation engineering.
Within this future landscape, large component adjustment represents more than repeated centrifugation. It becomes a scientific philosophy grounded in several core principles:
- biological information is fragile;
- specimen handling shapes analytical truth;
- pre-analytical precision influences translational validity;
- operational refinement reduces avoidable uncertainty;
- and reliable medicine begins long before analysis itself.
The second spin ultimately symbolises a commitment to protecting biological meaning during its most vulnerable transition—from living inflammatory physiology into measurable scientific evidence.
Long before a biomarker becomes a number, it must first survive the laboratory process intact enough to remain truthful.
CHAPTER 13
BIOSPECIMEN STABILITY, FREEZE-THAW DYNAMICS, AND LONG-TERM PLASMA INTEGRITY
One of the most misunderstood aspects of laboratory medicine is the assumption that biological specimens become stable once they are placed into storage. To those outside laboratory science, freezing plasma may appear to function as a form of biological suspension in which molecular activity simply stops entirely until future analysis occurs. In reality, biospecimen preservation is considerably more complex. Freezing slows degradation dramatically, but it does not erase the consequences of earlier handling conditions, nor does it fully eliminate all risks to biomarker integrity over time.
The life of a plasma specimen does not end after centrifugation.
In many ways, it begins there.
Within clinical trial laboratories, especially those involved in allergy and immunology research, plasma often enters long-term storage following initial processing. Samples may remain frozen for months or years before downstream biomarker analysis occurs. Some specimens become part of large biobanking infrastructures supporting future translational studies beyond the original aims of the clinical trial itself.
Consequently, the quality of pre-analytical preparation becomes deeply connected to the future scientific usefulness of the specimen.
Large component adjustment through repeated spinning plays a particularly important role within this broader framework of long-term biospecimen stability.
The objective of repeated centrifugation is not only to improve immediate analytical clarity but also to reduce biological instability capable of continuing during storage conditions. Residual platelets, leukocytes, fibrin fragments, cellular microparticles, and inflammatory debris remaining within incompletely processed plasma may contribute to progressive degradation patterns over time, especially during freeze-thaw exposure.
This issue becomes increasingly significant in diseases such as Aspirin-Exacerbated Respiratory Disease (AERD), where inflammatory biomarkers are often highly sensitive, biologically dynamic, and vulnerable to environmental disturbance.
To understand why freeze-thaw stability matters so profoundly, it is necessary first to understand the molecular fragility of plasma itself.
Plasma is not merely a passive liquid medium. It contains thousands of biologically active components existing in highly interconnected molecular environments. Proteins, cytokines, antibodies, inflammatory mediators, enzymes, metabolites, hormones, lipids, and extracellular vesicles coexist simultaneously within dynamic equilibrium. Even after collection and freezing, many of these structures remain vulnerable to physical and biochemical disruption.
Temperature shifts influence molecular behaviour directly.
Proteins may denature under unstable thermal conditions. Cytokines may degrade gradually across repeated freeze-thaw cycles. Enzymatic activity may persist transiently during incomplete freezing or slow thawing processes. Residual cellular materials may rupture during freezing, releasing intracellular substances into plasma and altering biomarker composition artificially.
The laboratory therefore attempts not only to preserve biological material but to preserve molecular relationships within that material.
Repeated spinning contributes to this preservation partly by reducing the quantity of residual biological structures capable of destabilising plasma during storage.
Residual platelets are especially important in this context. Platelets contain numerous inflammatory mediators, growth factors, cytokines, and bioactive molecules stored within intracellular granules. During freezing and thawing, platelet disruption may release these substances into surrounding plasma unexpectedly, potentially altering biomarker measurements significantly.
Similarly, residual leukocytes remaining within plasma may undergo structural breakdown over time, releasing intracellular proteins, nucleic acids, and inflammatory contents capable of influencing downstream assays.
Cleaner plasma generated through repeated centrifugation therefore generally demonstrates improved long-term analytical stability.
This principle becomes particularly important in translational immunology where clinical trial samples are often analysed in batches rather than immediately after collection.
Batch analysis offers several scientific advantages. Running samples simultaneously reduces inter-assay variability and improves comparative consistency between patients or treatment groups. However, batch analysis also means that plasma may remain frozen for extended periods before downstream biomarker evaluation occurs.
The integrity of stored specimens therefore becomes essential for maintaining scientific reliability across time.
This temporal dimension fundamentally changes how laboratories must think about biospecimen quality.
The value of a specimen is no longer determined solely by its immediate usability. Instead, its value depends partly upon its capacity to remain biologically interpretable in the future. A high-quality specimen is one capable of surviving time without losing meaningful analytical information.
Large component adjustment should therefore be understood partly as a temporal stabilisation strategy.
The second spin is not simply about present clarity. It is about future resilience.
This concept of resilience is increasingly important within modern biomedical research.
A resilient biospecimen maintains structural and molecular stability despite storage duration, transportation, technological evolution, repeated analytical handling, and freeze-thaw exposure. The better the initial plasma refinement, the greater the likelihood that future analyses will still reflect meaningful biological conditions rather than storage-induced artefacts.
This issue has become especially relevant with the rise of biobanking.
Biobanks function as long-term repositories preserving human biospecimens for future scientific investigation. Plasma collected during contemporary clinical trials may later support studies involving technologies not yet available during initial collection. Future investigators may evaluate archived specimens for newly discovered cytokines, proteomic signatures, metabolomic profiles, genetic fragments, extracellular vesicles, or inflammatory pathways unknown at the time the specimens were originally processed.
The scientific life of a biospecimen therefore often extends far beyond its original purpose.
This gives laboratory preparation extraordinary long-term importance.
A specimen inadequately processed today may lose future scientific value permanently. Residual contamination, poor plasma refinement, inconsistent storage, or repeated uncontrolled freeze-thaw exposure may compromise biomarkers before future technologies ever have the opportunity to study them.
Conversely, carefully refined plasma may preserve molecular information capable of supporting discoveries decades later.
The laboratory therefore operates partly as a custodian of future scientific possibility.
Within AERD research, this custodial role carries particular significance because understanding of the disease continues evolving rapidly. New relationships between eosinophils, platelets, mast cells, cytokines, epithelial dysfunction, and lipid mediators continue emerging through ongoing translational studies. Archived plasma specimens processed under high-integrity conditions may later become invaluable resources for exploring inflammatory mechanisms impossible to measure currently.
Repeated spinning contributes to this future potential by improving baseline specimen quality before long-term storage begins.
Freeze-thaw dynamics themselves represent one of the most important yet underappreciated threats to biomarker stability.
Each freeze-thaw cycle introduces molecular stress into the specimen environment. Ice crystal formation may physically disrupt cellular structures and proteins. Thawing may temporarily reactivate enzymatic processes before complete temperature stabilisation occurs. Some cytokines remain relatively stable across limited freeze-thaw exposure, while others degrade substantially.
The effects are often analyte-specific.
Certain inflammatory proteins tolerate repeated freezing well. Others deteriorate rapidly after only one or two thaw cycles. Consequently, laboratory storage strategies must anticipate future analytical requirements carefully.
Aliquoting becomes critical in this context.
Rather than repeatedly thawing entire plasma samples for multiple analyses, laboratories often divide plasma into smaller aliquots immediately following centrifugation. Each aliquot may then undergo individual thawing as needed, reducing cumulative freeze-thaw exposure across the overall specimen inventory.
Repeated spinning improves aliquoting quality indirectly by generating cleaner plasma with reduced particulate interference prior to storage.
Operationally, however, maintaining long-term biospecimen integrity is highly demanding.
Ultra-low temperature freezers operating at -80°C require continuous monitoring. Temperature fluctuations may compromise years of stored research material. Backup power systems become essential because freezer failure may destroy irreplaceable clinical trial specimens rapidly.
Laboratories therefore develop extensive infrastructure around biospecimen preservation.
Alarm systems monitor temperature deviations continuously. Freezer inventories require precise organisation to minimise unnecessary door opening. Dry ice logistics support specimen transport between research sites. Chain-of-custody systems track specimen movement rigorously. Storage audits verify sample location and integrity regularly.
This operational infrastructure reflects recognition that biological information is fragile even after freezing.
The physical environment of long-term storage also shapes laboratory psychology significantly.
Freezer rooms often contain thousands of patient specimens preserved across years of clinical research. Each box may represent extensive patient participation, therapeutic experimentation, operational labour, and scientific investment. Personnel handling these specimens understand that many are irreplaceable.
Some samples originate from rare diseases.
Some represent unique therapeutic response windows.
Some may support future discoveries impossible to predict presently.
The laboratory therefore develops a relationship with time unlike many other scientific environments.
Specimens collected years earlier remain operationally active because their future scientific potential persists. A plasma aliquot processed carefully today may later influence biomarker discovery, therapeutic targeting, precision medicine algorithms, or translational immunology research decades later.
Large component adjustment contributes quietly to this continuity across time.
The second spin becomes part of an effort to preserve biological meaning against temporal degradation.
Importantly, future biomedical technologies will likely increase rather than decrease the importance of high-integrity biospecimen storage.
Ultra-sensitive analytical platforms continue evolving rapidly. Single-molecule detection systems, advanced proteomics, extracellular vesicle analysis, cell-free nucleic acid profiling, and machine learning biomarker discovery all require exceptionally stable biological inputs. Future technologies may detect forms of pre-analytical disturbance currently invisible to existing assays.
This means that specimen quality standards may continue rising over time.
Plasma considered acceptable under contemporary protocols may prove suboptimal under future ultra-sensitive analytical systems. Consequently, pre-analytical refinement strategies such as repeated spinning increasingly represent proactive investments in future analytical compatibility.
The future of precision immunology therefore depends partly upon biospecimen foresight.
Laboratories must prepare specimens not only for current technologies but also for scientific systems still emerging. This requires thinking of plasma not as disposable clinical material but as long-term informational infrastructure.
The concept of informational infrastructure is important here.
Within translational medicine, biospecimens function similarly to data archives. They preserve biological states across time, enabling future reinterpretation as scientific understanding evolves. However, unlike digital data, biological information remains vulnerable to physical degradation continuously.
The laboratory therefore becomes an environment dedicated to slowing informational decay.
Repeated centrifugation forms one part of this larger preservation architecture.
By reducing residual biological instability before storage, large component adjustment improves the likelihood that future analyses will still reflect meaningful physiological information rather than artefacts introduced during handling or degradation.
This preservation philosophy ultimately reshapes how clinical trial laboratories should be understood.
They are not merely processing centres moving specimens rapidly toward immediate analysis. They are biological preservation systems safeguarding molecular evidence across time.
Within this framework, the centrifuge becomes more than a preparatory instrument. It becomes part of a temporal bridge connecting present patient biology with future scientific interpretation.
The second spin therefore symbolises more than procedural refinement alone. It symbolises an effort to preserve the future interpretability of biological truth before time gradually erodes it.
CHAPTER 14
STANDARDISATION, REGULATION, AND BIOSPECIMEN GOVERNANCE
One of the defining characteristics of modern clinical research is that scientific credibility no longer depends solely upon discovery itself. In contemporary biomedical science, knowledge must also be reproducible, traceable, auditable, and operationally defensible. A biomarker finding is not considered reliable merely because it appears statistically significant. It must emerge through systems capable of demonstrating procedural consistency, specimen integrity, regulatory compliance, and methodological transparency across every stage of laboratory handling.
This requirement has transformed clinical trial laboratories into highly governed scientific environments.
Within allergy and immunology research involving diseases such as Aspirin-Exacerbated Respiratory Disease (AERD), governance becomes especially important because inflammatory biomarkers are highly sensitive to pre-analytical variability. The integrity of cytokine measurements, eosinophilic profiles, platelet-associated mediators, leukotriene pathways, and other inflammatory signals depends heavily upon standardised specimen handling.
Consequently, large component adjustment and repeated centrifugation cannot exist merely as informal laboratory preferences. For such processes to contribute meaningfully to translational medicine, they must eventually become integrated into broader frameworks of standardisation and operational governance.
This introduces an important question within modern laboratory science:
How can biological complexity be managed consistently across highly variable real-world clinical environments?
The answer lies partly in standardisation.
Standardisation refers to the deliberate development of procedural systems designed to reduce avoidable variability across specimen collection, handling, processing, storage, and analysis. The goal is not to eliminate biological diversity itself but to minimise procedural inconsistency capable of obscuring biological interpretation.
This distinction is critical.
Biological variability contains scientific value.
Procedural variability often does not.
Patients naturally differ in inflammatory behaviour, disease progression, immune response, medication exposure, and biomarker expression. These differences are meaningful and essential to translational research. However, variability introduced through inconsistent centrifugation, delayed processing, improper plasma transfer, or unstable storage conditions may distort interpretation without contributing useful scientific information.
Standardisation therefore attempts to protect authentic biology from avoidable operational noise.
Within clinical trial laboratories, this protection occurs through extensive procedural governance systems.
Standard operating procedures (SOPs) form the foundation of these systems. SOPs specify how specimens should be collected, labelled, transported, centrifuged, aliquoted, stored, thawed, documented, and ultimately analysed. Every stage of biospecimen handling becomes operationally codified.
For centrifugation specifically, SOPs may define:
- relative centrifugal force or RPM,
- spin duration,
- temperature conditions,
- rotor type,
- braking intensity,
- plasma transfer methods,
- acceptable processing timelines,
- aliquot volume specifications,
- and storage requirements following centrifugation.
Repeated spinning protocols similarly require precise definition if they are to remain scientifically reproducible.
Without standardisation, repeated centrifugation risks becoming inconsistently applied between operators, institutions, or studies. One laboratory may perform secondary spins gently while another uses substantially higher force. Plasma transfer timing may vary. Residual platelet reduction may differ significantly despite superficially similar procedures.
Such inconsistencies undermine interpretational reliability.
This becomes especially problematic in multicentre clinical trials involving geographically distributed laboratories.
Modern pharmaceutical studies frequently involve dozens or even hundreds of research sites across multiple countries. Biospecimens collected from patients in different institutions must ultimately contribute to unified datasets capable of supporting regulatory submission and therapeutic evaluation.
The challenge is enormous.
Different laboratories operate under varying staffing conditions, equipment models, environmental factors, operational cultures, and workflow pressures. Yet translational medicine requires that specimens processed across these diverse environments remain scientifically comparable.
Governance systems exist partly to create this comparability.
Good Clinical Practice (GCP) and Good Laboratory Practice (GLP) frameworks establish operational expectations designed to preserve scientific reliability and patient safety. These frameworks govern not only analytical methodologies but also pre-analytical handling processes because specimen integrity directly influences data validity.
Within regulated clinical research, documentation becomes inseparable from scientific credibility.
Every biospecimen must possess a traceable history.
Collection times are recorded.
Transport conditions are monitored.
Centrifugation timestamps are documented.
Operator identities are logged.
Freezer locations are tracked.
Temperature excursions are investigated.
Aliquot transfers are recorded.
This extensive documentation infrastructure reflects a core principle of translational science: data must remain operationally explainable.
A biomarker value without traceable handling history possesses limited regulatory credibility because hidden procedural variability may have influenced the result.
The laboratory therefore functions partly as an accountability system preserving the chain of biological evidence from patient collection to final analysis.
Large component adjustment enters this governance framework in important ways.
If repeated spinning improves plasma quality and biomarker stability significantly, then it cannot remain merely an informal optimisation strategy dependent solely upon individual operator judgement. It must eventually become standardisable, measurable, and reproducible within regulated laboratory systems.
This raises several scientific questions.
How many spins are optimal for specific biomarker classes?
What centrifugal forces preserve inflammatory analytes best while reducing residual platelets effectively?
How does repeated spinning affect long-term storage stability?
Do certain cytokines respond differently to plasma refinement conditions?
Can repeated centrifugation improve reproducibility across institutions?
These questions represent the transition from operational practice to formal methodological science.
Historically, many laboratory procedures evolved through practical experience before later undergoing systematic validation. Large component adjustment may represent a similar trajectory within translational immunology.
At present, many experienced laboratory professionals recognise empirically that repeated spinning often improves plasma clarity and downstream analytical consistency. However, future biomedical systems may increasingly require quantitative validation of these observations through controlled methodological studies.
This transition reflects a broader transformation occurring across modern laboratory medicine.
Pre-analytical handling is gradually shifting from a background technical process toward an actively researched scientific discipline.
The reasons for this shift are becoming increasingly clear.
As analytical technologies become more sensitive, pre-analytical variability exerts greater influence over final data quality. Ultra-sensitive cytokine assays, multiplex inflammatory platforms, proteomic systems, extracellular vesicle analysis, metabolomics, and machine learning biomarker modelling all depend heavily upon biospecimen integrity.
Consequently, regulatory science itself may increasingly focus on biospecimen quality assurance.
Regulatory agencies already recognise that poorly controlled pre-analytical conditions may compromise biomarker reliability. However, future therapeutic systems based heavily on molecular profiling and precision immunology will likely intensify this concern further.
Precision medicine requires precision biospecimens.
This relationship may eventually transform how laboratories are audited and evaluated.
Traditionally, laboratory regulation focused heavily on analytical instrumentation accuracy, calibration standards, and reporting systems. In the future, pre-analytical refinement protocols such as plasma purification strategies, platelet reduction methodologies, freeze-thaw minimisation practices, and biospecimen engineering approaches may receive greater regulatory attention.
The concept of biospecimen engineering is especially important here.
Biospecimen engineering refers to the deliberate design of handling systems aimed at preserving biological information optimally for advanced analytical environments. This approach treats specimen preparation itself as a strategic scientific process rather than passive technical routine.
Large component adjustment aligns closely with this emerging philosophy.
Repeated spinning reflects intentional refinement of plasma conditions to support high-integrity biomarker analysis. The laboratory becomes less a place of passive specimen storage and more an active environment shaping analytical reliability through operational optimisation.
Importantly, governance systems must balance standardisation against flexibility carefully.
Biological systems are inherently variable. Not all specimens behave identically during centrifugation. Some plasma samples separate cleanly after one spin. Others demonstrate persistent platelet haze, lipaemia, fibrin traces, or inflammatory turbidity requiring additional refinement.
Rigid standardisation alone may therefore sometimes conflict with biological reality.
Experienced laboratory personnel often recognise when specimens require operational adaptation beyond baseline protocols. This introduces a complex challenge within regulated laboratory systems:
How can laboratories preserve procedural consistency while still allowing scientifically informed flexibility?
The answer likely lies in structured adaptive governance.
Structured adaptive governance allows controlled procedural adjustment within predefined scientific boundaries. For example, laboratories may establish validated criteria under which additional centrifugation becomes permissible based on observable specimen characteristics or analytical requirements.
Such systems preserve both reproducibility and operational responsiveness simultaneously.
The human dimension remains important here as well.
Laboratory governance is often imagined purely bureaucratically through protocols, audits, and documentation systems. However, governance also depends fundamentally upon professional culture. Personnel must internalise procedural discipline not merely as compliance obligation but as scientific responsibility.
Within high-quality laboratories, precision becomes cultural as much as procedural.
Experienced professionals understand why timelines matter.
They understand why freezer doors should remain open briefly.
They understand why repeated freeze-thaw cycles threaten biomarker stability.
They understand why disturbing the buffy coat during plasma transfer matters.
They understand why the second spin may preserve analytical reliability.
This understanding transforms procedural compliance into scientific intentionality.
Operational culture therefore becomes one of the most powerful forms of quality control within laboratory systems.
In translational immunology, this culture is increasingly important because many inflammatory biomarkers exist at the edge of analytical detectability. Small procedural inconsistencies may influence interpretation substantially.
AERD research illustrates this clearly.
The disease involves highly interconnected inflammatory pathways where cytokine concentrations, eosinophilic behaviour, platelet activity, and leukotriene signalling may shift dynamically. Therapeutic investigations targeting these pathways depend upon reliable biomarker preservation. Regulatory decisions regarding investigational therapies may ultimately rely partly on these laboratory-generated datasets.
The consequences of specimen handling therefore extend far beyond the laboratory itself.
This broader impact transforms biospecimen governance into an ethical issue as well as a scientific one.
Patients participating in clinical trials contribute biological material with expectation that it will be handled responsibly and meaningfully. Pharmaceutical development relies upon trustworthy evidence. Future therapies depend upon reproducible science.
Laboratory governance systems exist partly to honour these responsibilities.
Repeated spinning, within this context, represents more than procedural optimisation. It reflects commitment toward preserving biological truth under increasingly demanding scientific conditions.
The second spin becomes an operational expression of care.
Care for specimen integrity.
Care for biomarker reliability.
Care for scientific reproducibility.
Care for future translational interpretation.
As precision medicine continues evolving, laboratories may increasingly become recognised not merely as analytical service environments but as central guardians of biomedical reliability.
Within this future, large component adjustment may eventually be understood not as optional refinement but as part of a larger scientific movement toward high-integrity biospecimen science.
The future of medicine will depend not only upon discovering new biomarkers or developing new therapies. It will also depend upon governing the pathways through which biological evidence becomes trustworthy enough to guide human health decisions.
Long before medicine becomes policy, approval, or treatment, it must first survive the discipline of the laboratory process intact.
CONCLUSION
THE SECOND SPIN AND THE FUTURE OF BIOLOGICAL TRUTH
Throughout the history of medicine, scientific progress has often been associated with moments of visible innovation. New therapies emerge. Diseases become classified differently. Technologies evolve. Analytical systems become faster, more sensitive, and more computationally sophisticated. Yet beneath every visible advancement exists another quieter process that determines whether biomedical knowledge remains trustworthy in the first place: the preservation of biological integrity.
This book began with a simple operational observation within the clinical trial laboratory environment — the repeated spinning of blood.
At first glance, centrifugation appears routine, almost mechanical in its familiarity. Blood enters the centrifuge. Components separate. Plasma is transferred. The specimen proceeds toward downstream analysis. However, as explored throughout these chapters, repeated spinning represents far more than technical repetition. It reflects a broader scientific philosophy grounded in the understanding that biological information is fragile, unstable, and continuously vulnerable to distortion once removed from the body.
Large component adjustment emerged within this discussion not merely as a laboratory technique but as a framework for thinking about biospecimen integrity itself.
The second spin became symbolic of refinement.
The third spin became symbolic of preservation.
Each stage reflected an attempt to reduce avoidable uncertainty within highly sensitive biomedical environments.
Within allergy and immunology research involving Aspirin-Exacerbated Respiratory Disease (AERD), this refinement carries particular importance because inflammatory biology is extraordinarily dynamic. Cytokines fluctuate. Eosinophilic pathways evolve. Platelets interact with leukocytes. Mast cells amplify inflammatory signalling. Biomarkers exist within complex and continuously changing molecular relationships.
The laboratory therefore does not simply process biological material passively. It intervenes at one of the most vulnerable stages of translational medicine: the transition between living physiology and measurable scientific evidence.
This transition became a central theme throughout this work.
Blood inside the body exists within regulated biological equilibrium. Outside the body, instability begins almost immediately. Cells remain metabolically active transiently. Proteins become vulnerable to degradation. Platelets continue responding to mechanical stimulation. Time itself gradually alters specimen composition.
The role of the clinical trial laboratory is therefore fundamentally preservational.
Repeated centrifugation contributes to preservation by improving plasma purity, reducing residual cellular contamination, minimising post-collection biological activity, and stabilising biospecimens for downstream analysis and long-term storage. The objective is not artificial perfection but the protection of authentic biological signal against procedural distortion.
Importantly, this book also argued that pre-analytical optimisation deserves recognition as an independent scientific discipline rather than merely technical preparation preceding “real” analysis.
Modern medicine increasingly depends upon highly sensitive molecular interpretation. Precision immunology, biomarker-driven therapeutics, artificial intelligence-assisted diagnostics, proteomics, metabolomics, and personalised medicine all require biospecimens of exceptional integrity. Sophisticated analytical technologies cannot fully compensate for compromised biological inputs.
No machine can restore biological truth already lost during handling.
This reality reshapes the strategic importance of laboratory science profoundly.
Clinical laboratories are no longer merely supportive environments operating quietly beneath visible healthcare systems. They are translational infrastructures responsible for protecting the reliability of biomedical evidence itself. Every therapeutic conclusion, biomarker trend, inflammatory profile, and clinical trial dataset ultimately depends upon operational precision occurring long before statistical analysis begins.
The centrifuge therefore occupies a surprisingly central position within the architecture of modern medicine.
It represents the point at which unstable biology first encounters scientific control.
Repeated spinning symbolises the recognition that precision is cumulative. Reliable knowledge does not emerge solely through advanced instrumentation or computational sophistication. It emerges gradually through disciplined operational care applied consistently across every stage of biospecimen handling.
This care is deeply human.
One of the most important themes throughout this book has been the invisible labour sustaining laboratory science. Behind every plasma aliquot exists human concentration, procedural discipline, observational expertise, physical endurance, and sustained attentiveness. Laboratory personnel operate within environments where even small inconsistencies may carry substantial downstream consequences.
Yet this labour often remains absent from visible scientific narratives.
Patients rarely see the laboratories processing their specimens. Research publications rarely capture the operational complexity underlying biospecimen preparation. The intellectual prestige of biomedical science often concentrates around analytical discoveries while overlooking the procedural systems preserving specimen integrity beforehand.
This invisibility should not be mistaken for insignificance.
Modern medicine depends profoundly upon the operational precision of clinical laboratory environments. Without stable biospecimens, biomarker interpretation weakens. Without biomarker reliability, translational medicine loses confidence. Without confidence, therapeutic advancement slows.
The future of biomedical science therefore depends partly upon recognising pre-analytical handling as foundational scientific infrastructure.
Within this future, large component adjustment may continue evolving from practical operational refinement into formal biospecimen engineering methodology. Repeated centrifugation protocols may become increasingly standardised, validated, and integrated into precision medicine frameworks as analytical sensitivity continues advancing.
Future technologies will likely demand even higher specimen quality than current systems.
Artificial intelligence models will require biologically reliable training data. Ultra-sensitive inflammatory assays will detect increasingly subtle molecular patterns. Precision immunology will depend upon highly stable biomarker environments. Biobanks will preserve specimens for analyses not yet imaginable.
The quality of tomorrow’s discoveries will therefore depend heavily upon the biospecimen decisions made today.
This gives the clinical trial laboratory an unusual relationship with time.
The laboratory does not merely support present science. It preserves future scientific possibility. Plasma processed carefully today may later contribute to discoveries years or decades beyond the original clinical trial itself. Every refined biospecimen becomes part of a larger archive of translational potential.
Repeated spinning thus becomes more than procedural repetition. It becomes an act of scientific foresight.
Ultimately, this book has argued for a broader rethinking of how biomedical evidence is understood. Scientific truth is not produced only at the moment of statistical analysis or technological measurement. It is shaped gradually across operational systems designed to protect biology from instability long enough for meaningful interpretation to occur.
The second spin symbolises this philosophy perfectly.
It reflects patience against haste.
Refinement against approximation.
Preservation against degradation.
Discipline against uncertainty.
Most importantly, it reflects the understanding that biological information deserves careful handling because human health decisions ultimately depend upon it.
In the quiet rotation of the centrifuge exists one of modern medicine’s most overlooked truths: before science becomes knowledge, biology must first survive the laboratory intact enough to remain truthful.
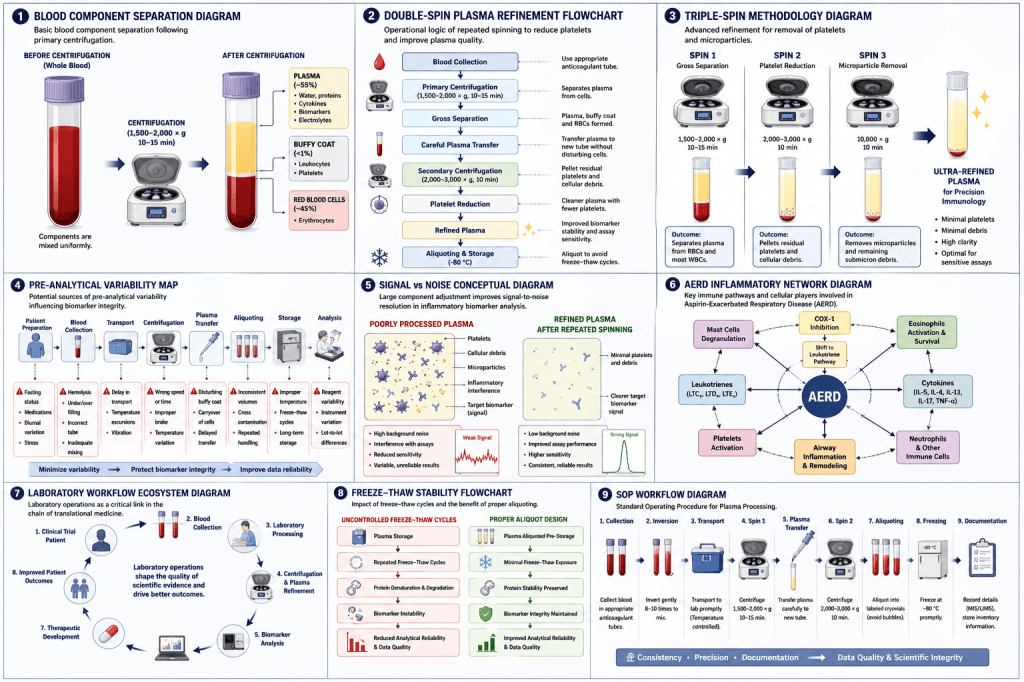
APPENDIX A
STANDARD OPERATING PROCEDURE (SOP)
| SOP Title | Double and Triple Spin Plasma Refinement Procedure for Immunological Biomarker Analysis |
| Document Number | [To be assigned] |
| Version | 1.0 |
| Effective Date | [Date] |
| Prepared By | Shahirah Izzati |
| Department | Clinical Trial Laboratory — Allergy & Immunology |
1. Purpose
To establish a standardised plasma processing workflow designed to improve biomarker integrity, reduce residual platelet contamination, and enhance analytical reliability within clinical trial laboratory environments.
2. Scope
This SOP applies to:
- allergy and immunology research studies;
- inflammatory biomarker analysis;
- AERD clinical trials;
- cytokine profiling;
- translational medicine research requiring high-integrity plasma.
3. Responsibilities
- Laboratory Scientist: specimen integrity, processing timelines, visual inspection;
- Senior Scientist / Supervisor: protocol oversight, deviation authorisation;
- Quality Assurance: documentation review, audit compliance;
- All Personnel: centrifuge calibration, storage compliance, chain-of-custody maintenance.
4. Equipment and Materials
| Equipment | Specification |
| Refrigerated centrifuge | Capable of 3,000 × g minimum; temperature control to 4°C |
| Calibrated pipettes | 100–1,000 µL range; verified calibration |
| Low-retention pipette tips | Sterile, individually wrapped |
| EDTA collection tubes | BD Vacutainer or equivalent |
| Labelled cryovials | 2 mL, screw-cap, barcoded |
| Ultra-low temperature freezer | −80°C monitored system with alarm |
| PPE | Gloves, lab coat, eye protection |
5. Step-by-Step Procedure
Step 1 — Sample Collection
- Collect blood using EDTA tubes;
- invert gently 8–10 times immediately;
- label tubes with patient ID, date, time;
- document collection time accurately.
Step 2 — Primary Centrifugation
- Place tubes in calibrated refrigerated centrifuge;
- balance rotor symmetrically;
- set parameters: 1,500–2,000 × g, 10–15 minutes, 4°C;
- use low brake during deceleration;
- record centrifugation start and end time.
Step 3 — Plasma Transfer
- Aspirate plasma carefully without disturbing buffy coat;
- stop aspiration 5–10 mm above buffy coat interface;
- transfer to clean labelled secondary tube;
- document transfer time.
Step 4 — Secondary Centrifugation
- Centrifuge transferred plasma at 2,000–3,000 × g, 10 minutes, 4°C;
- apply low braking;
- inspect plasma visually for clarity;
- record centrifugation parameters and timing.
Step 5 — Tertiary Centrifugation (Optional)
- Perform only for ultra-sensitive analytical applications;
- centrifuge at 3,000–5,000 × g, 10 minutes, 4°C;
- document rationale for tertiary spin in deviation or protocol log.
Step 6 — Aliquoting
- Divide plasma into labelled cryovials (200–500 µL per vial);
- record aliquot volumes and cryovial identifiers;
- complete chain-of-custody documentation.
Step 7 — Storage
- Store at −80°C in designated freezer location;
- record freezer ID, shelf, and box position;
- confirm storage in laboratory information system.
6. Deviation Management
Any deviation from this SOP must be:
- documented on a deviation report form;
- reviewed by the supervisor within 24 hours;
- assessed for impact on specimen integrity and downstream analysis;
- closed with corrective or preventive action where applicable.
7. References
- Lippi G et al. Preanalytical quality improvement. Clinical Chemistry and Laboratory Medicine.
- Laidlaw TM, Boyce JA. AERD. New England Journal of Medicine.
- de Jager W et al. Prerequisites for cytokine measurements. Clinical Immunology.
APPENDIX B
PLASMA HANDLING CHECKLIST
Complete this checklist for every specimen processed within the clinical trial laboratory.
| ✓ | Action |
| Pre-Collection | |
| ☐ | Patient fasting status confirmed and documented |
| ☐ | Collection timing confirmed relative to medication administration |
| ☐ | Inflammatory status / recent infection recorded |
| ☐ | Correct tube type selected for assay requirements |
| ☐ | Equipment (centrifuge, pipettes) verified and calibrated |
| Collection & Transport | |
| ☐ | Venepuncture performed — minimal tourniquet time |
| ☐ | Tubes inverted gently 8–10 times immediately |
| ☐ | Tubes labelled with patient ID, date, time |
| ☐ | Transport initiated within acceptable window |
| ☐ | Cold chain maintained during transport |
| Primary Centrifugation | |
| ☐ | Centrifuge pre-cooled to 4°C |
| ☐ | Rotor balanced symmetrically |
| ☐ | Parameters set: 1,500–2,000 × g, 10–15 min, 4°C |
| ☐ | Low braking applied |
| ☐ | Centrifugation start and end time documented |
| ☐ | Visual inspection completed — result recorded |
| Plasma Transfer | |
| ☐ | Plasma aspirated carefully without buffy coat disturbance |
| ☐ | Transfer completed to clean labelled secondary tube |
| ☐ | Transfer time documented |
| Secondary Centrifugation | |
| ☐ | Parameters set: 2,000–3,000 × g, 10 min, 4°C |
| ☐ | Low braking applied |
| ☐ | Timing documented |
| ☐ | Post-spin visual clarity assessed and recorded |
| Aliquoting & Storage | |
| ☐ | Plasma aliquoted into labelled cryovials (200–500 µL) |
| ☐ | Aliquot volumes and cryovial IDs recorded |
| ☐ | Specimens stored at −80°C in designated location |
| ☐ | Freezer position logged in laboratory system |
| ☐ | Chain-of-custody documentation completed |
| Operator Name | |
| Date | |
| Specimen ID | |
| Supervisor Review |
APPENDIX C
SAMPLE LABORATORY DOCUMENTATION FORMS
Sample documentation forms — including specimen receipt logs, centrifugation records, deviation reports, and chain-of-custody forms — should be developed in accordance with institutional SOPs, sponsor requirements, and applicable regulatory frameworks (GCP/GLP). Templates should be reviewed and approved by the Quality Assurance department prior to use.
APPENDIX D
BIOMARKER STABILITY REFERENCE TABLE
The following table provides general stability guidance for key inflammatory biomarkers relevant to AERD and allergy/immunology research. Values are approximate and may vary by assay platform, anticoagulant, and individual sample conditions. Always refer to manufacturer specifications.
| Biomarker | Class | Stability at RT | −20°C | −80°C | Freeze-Thaw Sensitivity |
| IL-4 | Cytokine | < 4 h | 6–12 months | > 2 years | High |
| IL-5 | Cytokine | < 4 h | 6–12 months | > 2 years | High |
| IL-13 | Cytokine | < 6 h | 6–12 months | > 2 years | Moderate-High |
| TNF-α | Cytokine | < 4 h | 3–6 months | > 1 year | High |
| IFN-γ | Cytokine | < 4 h | 6 months | > 2 years | Moderate |
| LTE4 | Leukotriene | < 2 h | 3–6 months | > 1 year | Very High |
| PGD2 | Prostaglandin | < 2 h | 3–6 months | > 1 year | Very High |
| Total IgE | Immunoglobulin | 24–48 h | > 2 years | > 5 years | Low |
| Tryptase | Enzyme | 8–12 h | 1–2 years | > 3 years | Low-Moderate |
| Eosinophil cationic protein | Eosinophil marker | 4–8 h | 1 year | > 2 years | Moderate |
RT = Room Temperature. Stability data based on published literature; individual assay validation is recommended.
REFERENCES
1. Lippi G, Chance JJ, Church S, et al. Preanalytical quality improvement: from dream to reality. Clinical Chemistry and Laboratory Medicine. 2011;49(7):1113–1126.
2. Plebani M. Errors in clinical laboratories or errors in laboratory medicine? Clinical Chemistry and Laboratory Medicine. 2006;44(6):750–759.
3. Bowen RAR, Remaley AT. Interferences from blood collection tube components on clinical chemistry assays. Biochemia Medica. 2014;24(1):31–44.
4. Rai AJ, Gelfand CA, Haywood BC, et al. HUPO Plasma Proteome Project specimen collection and handling. Proteomics. 2005;5(13):3262–3277.
5. Yin P, Peter A, Franken H, et al. Preanalytical aspects and sample quality assessment in metabolomics studies of human blood. Analytical Chemistry. 2013;85(21):10318–10325.
6. Laidlaw TM, Boyce JA. Aspirin-exacerbated respiratory disease — new prime suspects. New England Journal of Medicine. 2016;374(5):484–486.
7. Cahill KN, Boyce JA. Aspirin-exacerbated respiratory disease: mediators and mechanisms of a clinical disease. Journal of Allergy and Clinical Immunology. 2014;134(2):280–281.
8. Stevens WW, Schleimer RP, Kern RC. Chronic rhinosinusitis with nasal polyps. Journal of Allergy and Clinical Immunology: In Practice. 2016;4(4):565–572.
9. Bochenek G, Nizankowska E, Szczeklik A. Pathogenesis of aspirin-induced asthma and nasal polyps. Allergy. 1996;51(Suppl 30):28–36.
10. Kowalski ML. Aspirin-sensitive rhinosinusitis and asthma. Clinical Allergy and Immunology. 1999;13:215–235.
11. de Jager W, Bourcier K, Rijkers GT, et al. Prerequisites for cytokine measurements in clinical trials with multiplex immunoassays. Journal of Immunological Methods. 2009;347(1–2):1–14.
12. Flower L, Ahuja RH, Humphries SE, Mohamed-Ali V. Effects of sample handling on the stability of interleukin 6, tumour necrosis factor-alpha and leptin. Cytokine. 2000;12(11):1712–1716.
13. Aziz N, Nishanian P, Mitsuyasu R, et al. Variables that affect assays for plasma cytokines and soluble activation markers. Clinical Infectious Diseases. 1999;29(6):1344–1348.
14. Gros A, Ollivier V, Ho-Tin-Noe B. Platelets in inflammation: regulation of leukocyte activities and vascular repair. Frontiers in Immunology. 2014;5:678.
15. Semple JW, Italiano JE Jr, Freedman J. Platelets and the immune continuum. Nature Reviews Immunology. 2011;11(4):264–274.
16. Moore HM, Kelly AB, Jewell SD, et al. Biospecimen reporting for improved study quality (BRISQ). Cancer Cytopathology. 2011;119(2):92–101.
17. Vaught J, Kelly A, Hewitt R. A review of international biobanks and networks. Cancer Epidemiology, Biomarkers and Prevention. 2009;18(6):1660–1667.
18. Tuck MK, Chan DW, Chia D, et al. Standard operating procedures for serum and plasma collection. Journal of Proteome Research. 2009;8(1):113–117.
19. Collins FS, Varmus H. A new initiative on precision medicine. New England Journal of Medicine. 2015;372(9):793–795.
20. Fauci AS, Collins FS. Toward a new era of precision medicine. Annals of Internal Medicine. 2016;164(7):490–491.

Leave a comment